ņä£ ļĪĀ
Ēīīņóģņä▒ ĒÖ®ņāēņóģ(Xanthoma disseminatum)ņØĆ 1938ļģä MontgomeryņÖĆ OsterbergņŚÉ ņØśĒĢ┤ ņ▓śņØī ĻĖ░ņłĀ ļÉ£ ņ¦łĒÖśņ£╝ļĪ£ ņøÉņØĖņØä ņĢī ņłś ņŚåļŖö ļ¦żņÜ░ ļō£ļ¼Ė ļ╣ä ļ×æĻ▓īļź┤ĒĢ£ņŖż ņäĖĒż ņĪ░ņ¦üĻĄ¼ņ”Ø(Non-Langerhans cell histiocytosis)ņØ┤ļŗż[1]. ņĀüĒÖ®ņāē Ēś╣ņØĆ ņĀüĻ░łņāē ĻĄ¼ņ¦äņä▒ Ēö╝ļČĆ ļ│æļ│ĆņØ┤ ņ¢╝ĻĄ┤, ņŗĀņ▓┤ ĻĄ┤ņĖĪ ļČĆņ£ä ļ░Å ņĀÉļ¦ēņØä ņŻ╝ļĪ£ ņ╣©ļ▓ö ĒĢśļ®░ ļīĆļČĆļČäņØĆ ņ¢æņä▒ņØś Ļ▓ĮĻ│╝ļź╝ ļéśĒāĆļéĖļŗż. ĒĢśņ¦Ćļ¦ī ļ│æņØś ņ¦äĒ¢ē ņåŹļÅä ļ░Å ļ░£ņāØ ņ£äņ╣śņŚÉ ļö░ļØ╝ ņŗ¼Ļ░üĒĢ£ ĒĢ®ļ│æņ”ØĻ╣īņ¦Ć ņØ┤ņ¢┤ņ¦ł ņłś ņ׳ļŖöļŹ░ ņāüĻĖ░ļÅä ņ╣©ļ▓öņ£╝ļĪ£ ņØĖĒĢ£ ĒśĖĒØĪĻ│żļ×Ć, Ļ░üĻ▓░ļ¦ē ņ╣©ļ▓öņ£╝ļĪ£ ņØĖĒĢ£ ņŗżļ¬ģ, ņżæņČöņŗĀĻ▓ĮĻ│ä ņ╣©ļ▓öņŚÉ ņØśĒĢ£ Ļ░üņóģ ņŗĀĻ▓ĮņןņĢĀĻ░Ć ļ░£ņāØĒĢĀ ņłś ņ׳ļŗż[2].
Ēīīņóģņä▒ ĒÖ®ņāēņóģņØś ļ│æņØĖņØĆ ņĢäņ¦ü ļ¬ģĒÖĢĒ׳ ļ░ØĒśĆņĀĖ ņ׳ņ¦Ć ņĢŖļŗż. ļ╣ä ļ×æĻ▓īļź┤ĒĢ£ņŖż ņäĖĒżņØś ņĪ░ņ¦üĻĄ¼ņ”Ø ļ░Å ĻĘĖņŚÉ ļö░ļźĖ ņØ┤ņ░©ņĀüņØĖ ņ¦Ćņ¦łņØś ņČĢņĀüņŚÉ ņØśĒĢ£ Ļ▓āņØ┤ļØ╝Ļ│Ā ņāØĻ░üļÉśļéś ļīĆļČĆļČäņØś Ļ▓ĮņÜ░ ĒśłņĢĪĻ▓Ćņé¼ ņāü ņĀĢņāüņ¦Ćņ¦łĒśłņ”Ø ņåīĻ▓¼ņØä ļ│┤ņØĖļŗż[3]. Ēīīņóģņä▒ ĒÖ®ņāēņóģņØś ņ¦äļŗ©ņØĆ ņ×äņāüņĀü, ņĪ░ņ¦üĒĢÖņĀü, ļ®┤ņŚŁĒÖöĒĢÖņĀü ņåīĻ▓¼ņŚÉ ļö░ļØ╝ ļ│ĄĒĢ®ņĀüņ£╝ļĪ£ ņØ┤ļŻ©ņ¢┤ņ¦ĆĻ▓ī ļÉ£ļŗż. ņĪ░ņ¦üĒĢÖņĀüņ£╝ļĪ£ ļ”╝ĒöäĻĄ¼(lymphocyte), Ēżļ¦É ņĪ░ņ¦üĻĄ¼(foamy hsitiocyte), ļŗżĒĢĄĻ▒░ļīĆņäĖĒż(mutinuclear giant cell)ņØś ņ╣©ņ£żņØä ļ│┤ņØ┤ļ®░ ļ”╝ĒöäĻĄ¼ņÖĆ Ļ▒░ļīĆņäĖĒżņŚÉņä£ CD68ņŚÉ ļīĆĒĢ┤ ņ¢æņä▒ ņåīĻ▓¼ņØä ļ│┤ņØĖļŗż. ļśÉĒĢ£ ļ”╝ĒöäĻĄ¼ņÖĆ Ēżļ¦É ņĪ░ņ¦üĻĄ¼ņŚÉņä£ ļ░▒ĒśłĻĄ¼ Ļ│ĄĒåĄĒĢŁņøÉ(Leukocyte common antigen)ņŚÉ ļīĆĒĢ┤ ņ¢æņä▒ņåīĻ▓¼ņØä ļ│┤ņØ┤ļ®░ S-100, c-kitņŚÉ ļīĆĒĢ┤ņä£ļŖö ņØīņä▒ņåīĻ▓¼ņØä ļ│┤ņØĖļŗż.
ņ¦łĒÖś ļ░£ņāØņØś ļ╣łļÅäĻ░Ć ļō£ļ¼╝ĻĖ░ ļĢīļ¼ĖņŚÉ ņĢäņ¦üĻ╣īņ¦Ć ņĀĢĒÖĢĒĢ£ ņ╣śļŻīļ▓ĢņØ┤ ņĀĢĒĢ┤ņ¦Ćņ¦ĆļŖö ņĢŖņĢśļŗż. Ēśäņ×¼ ņØ┤ņŚÉ ļīĆĒĢ£ ņ╣śļŻīļĪ£ Ēü¼Ļ▓ī ņĀäņŗĀņ╣śļŻīņÖĆ ĻĄŁņåīņ╣śļŻīļĪ£ ļéśļłäņ¢┤ ļ│╝ ņłś ņ׳ņ£╝ļ®░ ņĀäņŗĀņ╣śļŻīļĪ£ļŖö fenofibrate, statin, PPAR-╬│ņÖĆ Ļ░ÖņØĆ ņ¦Ćņ¦łĻ░ĢĒĢśņĀ£, cyclophosphamide, cyclosporine ļō▒ņØś ļ®┤ņŚŁņ¢ĄņĀ£ņĀ£, ĻĘĖļ”¼Ļ│Ā steroid, doxycycline, chlorodeoxyadenosine ļō▒ņØä ņé¼ņÜ®ĒĢ┤ ņÖöņ£╝ļéś ļ¬ģĒÖĢĒĢ£ ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝ņ¦ĆļŖö ļ¬╗ĒĢśņśĆļŗż[4,5]. ĻĄŁņåīņĀü ņ╣śļŻīļĪ£ļŖö ļāēļÅÖņ╣śļŻī, ļ░®ņé¼ņäĀņ╣śļŻī, CO2 laser, ļ│æļ│ĆņØś ņłśņłĀņĀü ņĀłņĀ£ ļō▒ņØ┤ ņŗ£ļÅäļÉśņŚłĻ│Ā ļŗżņ¢æĒĢ£ Ļ▓░Ļ│╝Ļ░Ć ļ│┤Ļ│ĀļÉśņŚłļŗż[6].
ņĀĆņ×ÉļōżņØĆ ņØ┤ļ╣äņØĖĒøäĻ│╝ņśüņŚŁņŚÉņä£ ĒØöņ╣ś ņĢŖņØĆ ĒøäļæÉņØś Ēīīņóģņä▒ ĒÖ®ņāēņóģņØä Ļ▓ĮĒŚśĒĢśņśĆĻĖ░ņŚÉ ĻĖ░ņĪ┤ ļ¼ĖĒŚī Ļ│Āņ░░Ļ│╝ ĒĢ©Ļ╗ś ņ”ØļĪĆļ│┤Ļ│Āļź╝ ĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ņ”Ø ļĪĆ
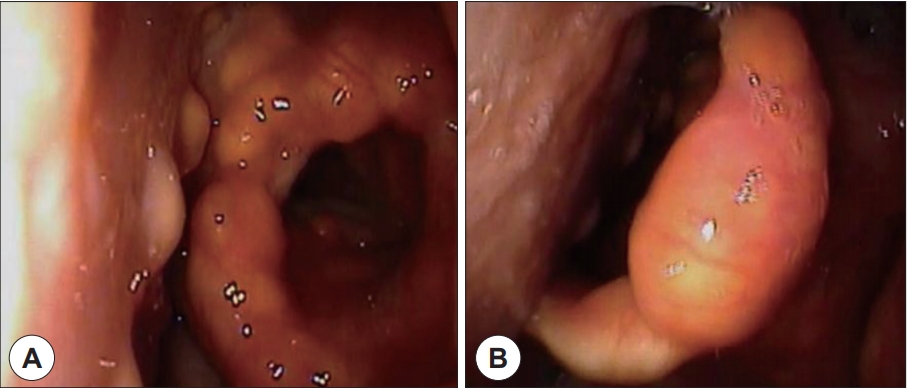
59ņäĖ ļé©ņ×É ĒÖśņ×ÉĻ░Ć 2ļŗ¼ ņĀäļČĆĒä░ ļéśĒāĆļé£ ĒśĖĒØĪ ļ░Å ņé╝Ēé┤ ņŗ£ ļČłĒÄĖĻ░ÉņØä ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢśņśĆļŗż. ļé┤ņøÉ ļŗ╣ņŗ£ ĒÖśņ×ÉļŖö ĒśłņĢĪ Ļ▓Ćņé¼ ņāü ņé░ņåī ĒżĒÖöļÅä ņĀĆĒĢś ļ░Å ņĀĆņé░ņåīĒśłņ”Ø ņåīĻ▓¼ņØĆ ņŚåņŚłņ£╝ļéś ĒśĖĒØĪ ņŗ£ ļČłĒÄĖĻ░É, ņé╝Ēé┤ ņŗ£ ņØ┤ļ¼╝Ļ░É ļ░Å Ļ▓Įļ»ĖĒĢ£ ņØīņä▒ ļ│ĆĒÖöļź╝ ĒśĖņåīĒĢśĻ│Ā ņ׳ņŚłļŗż. ņŗĀņ▓┤ ņ¦äņ░░ ņāü ņ¢æņĖĪ ļłł, ņĮö, ņ×ģņłĀ ņŻ╝ņ£äņÖĆ ļ¬®, ņ¢æņ¬Į Ļ▓©ļō£ļ×æņØ┤, ņé¼ĒāĆĻĄ¼ļŗł ļ░Å ĻĄ¼Ļ░Ģ ļé┤ ņĀÉļ¦ēņŚÉ ĒÖ®Ļ░łņāēņØś ļŗżļ░£ņä▒ ĻĄ¼ņ¦äņä▒ Ēö╝ļČĆ ļ│æļ│ĆņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 1).
ņØ┤ņŚÉ ņĢ×ņä£ 2ļģä ņĀäļČĆĒä░ ļéśĒāĆļé£ ņ¢╝ĻĄ┤Ļ│╝ ļ¬®, ņ¢æņĖĪ Ļ▓©ļō£ļ×æņØ┤, ņé¼ĒāĆĻĄ¼ļŗłņØś ļŗżļ░£ņä▒ ĻĄ¼ņ¦äņ£╝ļĪ£ ĒāĆļ│æņøÉ Ēö╝ļČĆĻ│╝ ņ¦äļŻīļź╝ ļ│┤ņĢśņ£╝ļ®░ Ēö╝ļČĆņĪ░ņ¦üĻ▓Ćņé¼ ņāü Ēīīņóģņä▒ ĒÖ®ņāēņóģņ£╝ļĪ£ ņ¦äļŗ© ļ░øņĢśņ£╝ļéś ļ│äļŗżļźĖ ņ╣śļŻīļŖö ļ░øĻ│Ā ņ׳ņ¦Ć ņĢŖņĢśļŗż. ņ×ģņøÉ ĻĖ░Ļ░ä ļÅäņżæ ļ│ĖņøÉ Ēö╝ļČĆĻ│╝ņŚÉņä£ Ēö╝ļČĆ ļ│æļ│ĆņŚÉ ļīĆĒĢ£ ņĪ░ņ¦üĻ▓Ćņé¼ļź╝ ļŗżņŗ£ ņŗ£Ē¢ēĒĢśņśĆĻ│Ā Ēīīņóģņä▒ ĒÖ®ņāēņóģņ£╝ļĪ£ ņ×¼ņ░© ņ¦äļŗ© ļ░øņĢśļŗż.
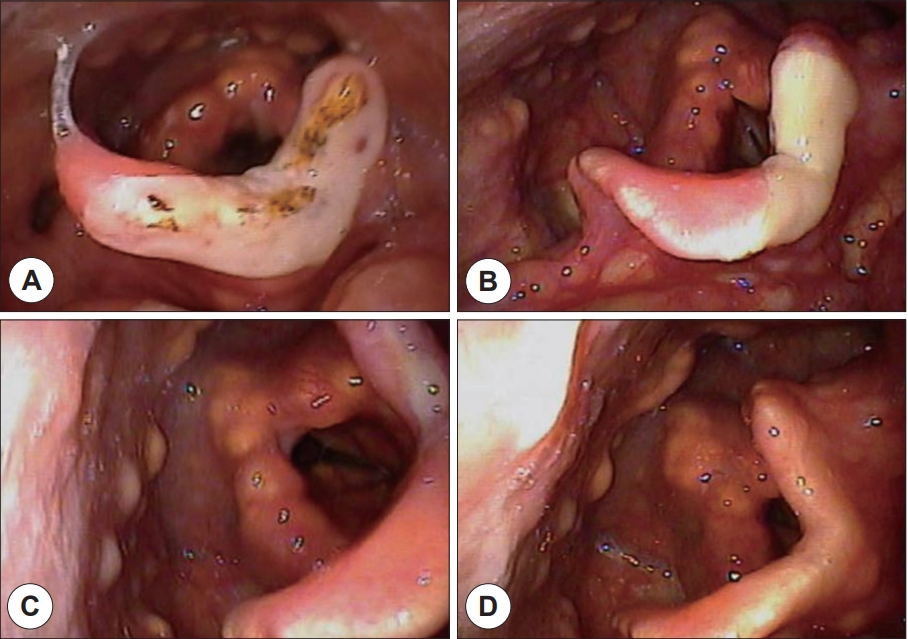
ĒøäļæÉļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ņŚÉņä£ ņ¢æņĖĪ Ēö╝ņŚ┤ņŚ░Ļ│©, Ēö╝ņŚ┤ĒøäļæÉĻ░£ņŻ╝ļ”ä, ĒøäļæÉĻ░£ ļ░Å ĒĢśņØĖļæÉ ņĀÉļ¦ēņØś ļŗżļ░£ņä▒ņØś ĒÖ®ņāē Ļ▓░ņĀłņä▒ ļ│æļ│ĆņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż. ĒŖ╣Ē׳ ĒøäļæÉĻ░£ ņāüļČĆņŚÉņä£ļŖö 2 cm Ēü¼ĻĖ░ņØś ļ╣äĻĄÉņĀü Ēü░ ļ│æļ│ĆņØ┤ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░ ĒÖśņ×ÉņØś ņ”ØņāüņØä ņØ╝ņ£╝ĒéżļŖö Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉśņŚłļŗż(Fig. 2). ĒÖ®ņāē Ļ▓░ņĀłņä▒ ļ│æļ│ĆņØĆ Ļ░Ćņä▒ļīĆ ļ░Å ņ¦äņä▒ļīĆņØś ņĀÉļ¦ēņŚÉņä£ļŖö Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░ ņä▒ļīĆņØś ņøĆņ¦üņ×äņŚÉļŖö ņØ┤ņāüņØ┤ ņŚåņŚłļŗż.
ĒśłņĢĪĻ▓Ćņé¼ ņāü Triglyceride 156 mg/dL, total cholesterol 158 mg/dL, LDL cholesterol 82 mg/dLļĪ£ ņĀĢņāü ņ¦Ćņ¦łĒśłņ”ØņØś ņåīĻ▓¼ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż. AST 83 IU/L, ALT 71 IU/L, Serum creatinine 2.1 mg/dL, BUN 21.0 mg/dLņ£╝ļĪ£ Ļ░ä, ņŗĀĻĖ░ļŖź ņĀĆĒĢśĻ░Ć Ļ┤Ćņ░░ļÉśņŚłĻ│Ā ĒøäļæÉļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ņŚÉņä£ ļ│æļ│ĆņØś Ļ╣ŖņØ┤Ļ░Ć ņĀÉļ¦ēĒĢśņĖĄņŚÉ ĻĄŁĒĢ£ļÉśņ¢┤ ņ׳ļŖö Ļ▓āņ£╝ļĪ£ ĒīÉļŗ©ļÉśņŚłĻĖ░ ļĢīļ¼ĖņŚÉ Ļ▓ĮļČĆņ╗┤Ēō©Ēä░ļŗ©ņĖĄņ┤¼ņśü(Computed tomography)ļŖö ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņĢśļŗż.
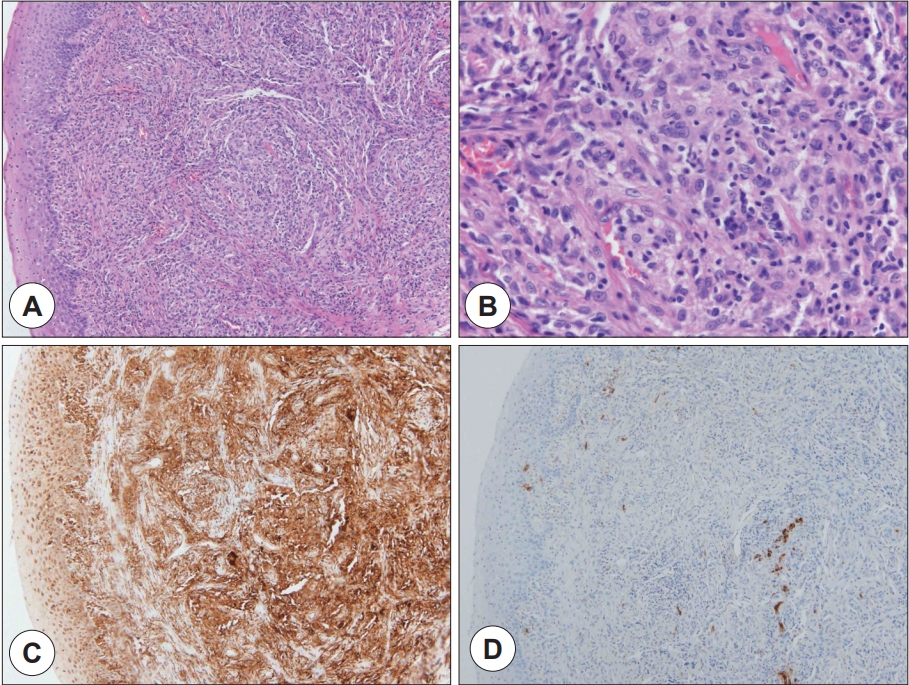
ĒøäļæÉļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ņŚÉņä£ Ļ┤Ćņ░░ ļÉ£ ĒøäļæÉĻ░£ ņāüļČĆņØś 2 cm Ēü¼ĻĖ░ņØś Ļ▓░ņĀłņä▒ ļ│æļ│ĆņØ┤ ĒÖśņ×ÉņØś ņ”ØņāüĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉśņ¢┤ ņłśņłĀņĀü ņĀłņĀ£ļź╝ Ļ│äĒÜŹĒĢśņśĆļŗż. ĒśäņłśĒøäļæÉĻ▓ĮņØä ņØ┤ņÜ®ĒĢ£ Ļ▓ĮĻĄ¼Ļ░ĢņĀü ņĀæĻĘ╝ļ▓ĢņØä ĒåĄĒĢ┤ ĒøäļæÉĻ░£ ņóģĻ┤┤ņØś ņłśņłĀņĀü ņĀ£Ļ▒░ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. CO2 ļĀłņØ┤ņĀĆļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņóģĻ┤┤ņØś Ļ▓ĮĻ│äļź╝ ĒÖĢņØĖĒĢśļ®░ ņĪ░ņŗ¼ņŖżļ¤ĮĻ▓ī ļ░Ģļ”¼ļź╝ ĒĢśņśĆļŗż. ņóģĻ┤┤ļŖö ņŻ╝ļ│Ć ņĪ░ņ¦üņŚÉ ņ£Āņ░® ņŚåņØ┤ ļ╣äĻĄÉņĀü ņēĮĻ▓ī ņĀłņĀ£ļÉśņŚłņ£╝ļ®░ ņČ£ĒśłņØ┤ļéś ņŗ¼ĒĢ£ ĒøäļæÉĻ░£ ļČĆņóģņØĆ ļ░£ņāØĒĢśņ¦Ć ņĢŖņĢśļŗż.. ņłśņłĀ Ēøä 3ņØ╝ņ¦Ė ļ│äļŗżļźĖ ĒĢ®ļ│æņ”Ø ņŚåņØ┤ Ēć┤ņøÉĒĢśņśĆĻ│Ā ņÖĖļל ņČöņĀüĻ┤Ćņ░░ ĒĢśņśĆļŗż. ļé┤Ļ│╝ņĀüņ£╝ļĪ£ļŖö ņ¦Ćņ¦łĻ░ĢĒĢśņĀ£(statin)ļź╝ ļ│ĄņÜ®ĒĢśļ®░ Ļ▓ĮĻ│╝Ļ┤Ćņ░░ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņłśņłĀ Ēøä ņŗ£Ē¢ēĒĢ£ ņĪ░ņ¦üĻ▓Ćņé¼ņŚÉņä£ H&E ņŚ╝ņāēņŚÉņä£ ļ”╝ĒöäĻĄ¼, Ēżļ¦É ņĪ░ņ¦üĻĄ¼ ļō▒ņØś ņ╣©ņ£żņØ┤ Ļ┤Ćņ░░ ļÉśņŚłņ£╝ļ®░ CD68ņŚÉ ļīĆĒĢśņŚ¼ ņ¢æņä▒ ņåīĻ▓¼, S-100ņŚÉ ļīĆĒĢ┤ņä£ļŖö ņØīņä▒ņåīĻ▓¼ņØä ļ│┤ņŚ¼ Ēīīņóģņä▒ ĒÖ®ņāēņóģņ£╝ļĪ£ ņ¦äļŗ©ĒĢĀ ņłś ņ׳ņŚłļŗż(Fig. 3). ņłśņłĀņĀü ņ╣śļŻī ņŗ£Ē¢ē Ēøä 2ņŻ╝, 1ļŗ¼ ņ¦Ė ņÖĖļל ļé┤ņøÉĒĢśņśĆņ£╝ļ®░ ĒÖśņ×ÉļŖö ĒśĖĒØĪĻ│żļ×Ć, ņé╝Ēé┤Ļ│żļ×Ć ļō▒ņØś ņ”ØņāüņØä ĒśĖņåīĒĢśņ¦Ć ņĢŖņĢśĻ│Ā ĒøäļæÉļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ ņāü ĒĢ®ļ│æņ”Ø ļ░Å ņ×¼ļ░£ ņåīĻ▓¼ņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż. ņłśņłĀ 6Ļ░£ņøö Ēøä, ĒøäļæÉļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ņŚÉņä£ Ļ▓░ņĀłņä▒ ļ│æļ│ĆņØś ņ¦äĒ¢ēņØĆ ļŹöņØ┤ņāü Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░ ĒśĖĒØĪĻ│żļ×Ć ļō▒ņØś ņ”Øņāü ļśÉĒĢ£ ĒśĖņåīĒĢśņ¦Ć ņĢŖņĢśļŗż(Fig. 4).
Ļ│Ā ņ░░
Ēīīņóģņä▒ ĒÖ®ņāēņóģņØĆ ņĀĢņāüņ¦Ćļ░®Ēśłņ”ØņØś ļ╣ä ņ£ĀņĀäņä▒ ņĀÉļ¦ē Ēö╝ļČĆ ņ¦łĒÖśņØ┤ļŗż. ļ¼ĖĒŚī ņāü 100ņśłĻ░Ć ļ│┤Ļ│ĀļÉĀ ņĀĢļÅäļĪ£ ļ¦żņÜ░ ļō£ļ¼Ė ņ¦łĒÖśņ£╝ļĪ£ 60%ņŚÉņä£ 25ņäĖ ņØ┤ņĀäņŚÉ, ņŻ╝ļĪ£ ļé©ņä▒ņŚÉņä£ ĒśĖļ░£ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[7,8]. ņĀüĒÖ®ņāē Ēś╣ņØĆ ņĀüĻ░łņāēņØś ĻĄ¼ņ¦äņä▒ Ēö╝ļČĆ ļ│æļ│ĆņØ┤ ņŻ╝ļĪ£ ņ¢╝ĻĄ┤, ņŗĀņ▓┤ ĻĄ┤ņĖĪļČĆ ļō▒ņØä ņ╣©ļ▓öĒĢśļ®░ 40~60%ņŚÉņä£ ĻĄ¼ņØĖļæÉ, ĒøäļæÉ ļ░Å Ļ▓░ļ¦ē, Ļ░üļ¦ē ļō▒ņØä ņ╣©ļ▓öĒĢ£ļŗż. ņŻ╝ļĪ£ ņ¢æņä▒ņØś Ļ▓ĮĻ│╝ļź╝ ļéśĒāĆļé┤ļéś ņ╣©ļ▓öĒĢ£ ļ│æļ│ĆņØś ĒĢ┤ļČĆĒĢÖņĀü ņ£äņ╣śļéś ļ│æļ│ĆņØś ņ¦äĒ¢ē ņåŹļÅäņŚÉ ļö░ļØ╝ ņŗ¼Ļ░üĒĢ£ ĒĢ®ļ│æņ”ØņØä ņ┤łļלĒĢĀ ņłś ņ׳ļŗż[9]. ĻĄ¼ņØĖļæÉ ļ░Å ĒøäļæÉņŚÉ ņ╣©ļ▓öĒ¢łņØä Ļ▓ĮņÜ░ ņŚ░ĒĢśĻ│żļ×Ć ļ░Å ĒśĖĒØĪĻ│żļ×Ć ļō▒ņØä ĒśĖņåīĒĢĀ ņłś ņ׳ņ£╝ļ®░ Ļ▓░ļ¦ē ļ░Å Ļ░üļ¦ē ņ╣©ļ▓ö ņŗ£ ņŗ£ņĢ╝ ļ░Å ņŗ£ļĀźņŚÉ ņןņĢĀĻ░Ć ņāØĻĖĖ ņłś ņ׳ļŗż. ņØ┤ņÖĖņŚÉļÅä ļō£ļ¼╝Ļ▓ī ņżæņČöņŗĀĻ▓ĮĻ│ä ļ░Å ĒśĖĒØĪĻĖ░Ļ│äļź╝ ņ╣©ļ▓öĒĢśļŖö Ļ▓ĮņÜ░ļÅä ņ׳ņ£╝ļ®░ ņØ┤ļŖö ņ╣śļ¬ģņĀüņØĖ Ļ▓░Ļ│╝ļź╝ ņĢ╝ĻĖ░ĒĢśĻĖ░ļÅä ĒĢ£ļŗż[10,11].
Ēīīņóģņä▒ ĒÖ®ņāēņóģņØś ņĪ░ņĀł ļ░Å ņ╣śļŻīļź╝ ņ£äĒĢ┤ ļ¦ÄņØĆ ņĀäņŗĀņĀü ņ╣śļŻīņĀ£ļōżņØ┤ ņé¼ņÜ®ļÉśņ¢┤ ņÖöņ£╝ļéś ņĢäņ¦üĻ╣īņ¦Ć ĒÖĢļ”ĮļÉ£ ņ╣śļŻīļ▓ĢņØĆ ļ│┤Ļ│ĀļÉśņ¦Ć ņĢŖņĢśļŗż. Ēīīņóģņä▒ ĒÖ®ņāēņóģņØś ņĀäņŗĀņĀü ņ╣śļŻīļĪ£ ļīĆļČĆļČäņØ┤ ņŖżĒģīļĪ£ņØ┤ļō£ ļ░Å ļ®┤ņŚŁņ¢ĄņĀ£ņĀ£ļź╝ ņé¼ņÜ®ĒĢśņśĆņ£╝ļéś ņ╣śļŻīņŚÉ ļ░śņØæņØä ļ│┤ņØĖ Ļ▓ĮņÜ░ļŖö ļō£ļ¼╝ļŗżĻ│Ā ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż. ĻĘĖ ļ░¢ņØś ņ╣śļŻīņĀ£ļĪ£ ĒĢŁĻ│Āņ¦ĆĒśłņ”ØņĀ£ Ēś╣ņØĆ azathioprineĻ│╝ cyclophosphamideņØś ļ│æņÜ®ņÜöļ▓Ģ, clofibrateņÖĆ ĒĢŁņĢöņ╣śļŻīņØś ļ│æņÜ®ņÜöļ▓ĢņØ┤ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ņŚłņ£╝ļ®░[12], ĒŖ╣Ē׳ļéś Ēö╝ļČĆ ļ│æļ│ĆņØś ņןĻĖ░ņĀüņØĖ Ļ┤ĆĒĢ┤ļź╝ ņ£Āņ¦ĆĒĢśļŖöļŹ░ 2-chlorodeoxyadenosineĻ░Ć ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗżļŖö ļ│┤Ļ│ĀļÅä ņ׳ņŚłļŗż[13]. ņĄ£ĻĘ╝ ĒĢŁĻ│Āņ¦ĆĒśłņ”ØņĀ£ņØĖ fenofibrate, statin, PPAR-╬│ļź╝ ļ│æņÜ®ĒĢśņśĆņØä ļĢī ļ│æļ│ĆņØś 50% ņØ┤ņāüņØś ĒśĖņĀäņØä ļ│┤ņśĆļŗżļŖö ņ”ØļĪĆļ│┤Ļ│ĀĻ░Ć ņ׳ņŚłņ£╝ļéś 3ļģäņØś Ļ▓ĮĻ│╝Ļ┤Ćņ░░ ĻĖ░Ļ░ä ļÅÖņĢł ņÖäņĀäĒĢ£ Ļ┤ĆĒĢ┤ļŖö Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż[14].
Ēīīņóģņä▒ ĒÖ®ņāēņóģņØś ĻĄŁņåīņ╣śļŻīļĪ£ ļŗżņ¢æĒĢ£ ļ░®ļ▓ĢļōżņØ┤ ņØ┤ņÜ®ļÉśņ¢┤ ņÖöņ£╝ļ®░ ļŗżņ¢æĒĢ£ Ļ▓░Ļ│╝ļź╝ ļéśĒāĆļé┤ņŚłļŗż. Ļ│╝Ļ▒░ņŚÉļŖö ņØĖļæÉ, ĒøäļæÉ, ĻĖ░Ļ┤Ć ļō▒ņŚÉ ņ╣©ļ▓öĒĢ£ ļ│æļ│ĆņØś ņĪ░ņĀłņØä ņ£äĒĢ┤ ļ░®ņé¼ņäĀ ņ╣śļŻīļź╝ ņŗ£ļÅäĒĢ£ Ļ▓ĮņÜ░ļÅä ņ׳ņŚłņ£╝ļéś ĻĘĖ ņłśĻ░Ć ņĀüņ¢┤ ĒÜ©Ļ│╝Ļ░Ć ļ¬ģĒÖĢĒĢśĻ▓ī ļ░ØĒśĆņ¦Ćņ¦Ć ņĢŖņĢśļŗż. ļ│æļ│ĆņØ┤ ņ”ØņāüĻ│╝ņØś ņŚ░Ļ┤Ćņä▒ņØ┤ ļ¬ģĒÖĢĒĢśĻ│Ā ņłśņłĀņĀü ņĀłņĀ£Ļ░Ć Ļ░ĆļŖźĒĢ£ Ļ▓ĮņÜ░ ņłśņłĀņĀü ņĀłņĀ£ļŖö ļ╣äĻĄÉņĀü ĒÖĢņŗżĒĢ£ ĒÜ©Ļ│╝ņØś ņ╣śļŻīļ▓ĢņØ┤ ļÉĀ ņłś ņ׳ļŗż[15,16]. ņłśņłĀņĀü ņĀłņĀ£Ļ░Ć ņ¢┤ļĀżņÜ┤ Ļ▓ĮņÜ░, ĒŖ╣Ē׳ ņĀäņŗĀņĀüņ£╝ļĪ£ Ēö╝ļČĆļ│æļ│ĆņØ┤ ĒŹ╝ņĀĖ ņ׳ļŖö Ļ▓ĮņÜ░ CO2 laserĻ░Ć ļīĆņĢłņĀüņØĖ ņ╣śļŻī ļ░®ļ▓ĢņØ┤ ļÉĀ ņłś ņ׳ņŚłņ£╝ļ®░ ņØ┤ņÖĖņŚÉļÅä ļāēļÅÖņ╣śļŻī, ļ│æļ│Ć ļé┤ ņŖżĒģīļĪ£ņØ┤ļō£ ņŻ╝ņ×ģņłĀ, ņĀäĻĖ░ņåīņ×æņłĀ, ļ░ĢĒö╝ņłĀ ļō▒ņØś ņ╣śļŻīļ▓ĢņØ┤ ņŗ£ļÅäļÉ£ Ļ▓ĮņÜ░Ļ░Ć ņ׳ņŚłļŗż[17,18].
ļ│Ė ņ”ØļĪĆņŚÉņä£ļŖö ņĀäĒśĢņĀüņØĖ ĒÖ®ņāē ĻĄ¼ņ¦äņä▒ ļ│æļ│ĆņØ┤ ņĀäņŗĀņŚÉ Ļ▒Ėņ│É ņ╣©ļ▓öĒĢśņśĆĻ│Ā ĻĄ¼Ļ░Ģ ņĀÉļ¦ēĻ│╝ ĒĢśņØĖļæÉ ļ░Å ĒøäļæÉņØś ņĀÉļ¦ēņØä ņ╣©ļ▓öĒĢśņśĆļŗż. ĒŖ╣Ē׳ ĒøäļæÉĻ░£ ņāüļČĆņŚÉņä£ 2 cm Ēü¼ĻĖ░ņØś Ļ▓░ņĀłņä▒ ņóģĻ┤┤Ļ░Ć Ļ┤Ćņ░░ļÉśņŚłĻ│Ā ņØ┤ļĪ£ ņØĖĒĢ┤ ĒśĖĒØĪĻ│żļ×Ć ļ░Å ņé╝Ēé┤ Ļ│żļ×Ć ļō▒ņØś ņ”ØņāüņØ┤ ļéśĒāĆļéśļŖö Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉśņŚłļŗż. ņØ┤ņÖĆ Ļ░ÖņØ┤ ĻĖ░ļÅäĒÅÉņāē ņ”ØņāüņØä ņØ╝ņ£╝ĒéżļŖö Ļ▓ĮņÜ░, Ēś╣ņØĆ ĻĖ░ļÅä ĒÅÉņāēņØ┤ ņśłņāüļÉśļŖö Ļ▓ĮņÜ░ Ēü¼ĻĖ░ ļ│ĆĒÖö ļ░Å ņ”ØņāüņŚÉ ļīĆĒĢ£ ņŻ╝ņØś Ļ╣ŖņØĆ Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ņØ┤ ĒĢäņÜöĒĢśļ®░ ņ×¼ļ░£ ņŚ¼ļČĆņÖĆ ņāüĻ┤Ć ņŚåņØ┤ ņłśņłĀņĀü ņĀłņĀ£Ļ░Ć ĒĢäņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.
ļ│Ė ņ”ØļĪĆņŚÉņä£ļŖö ļ│æļ│ĆņŚÉ ļīĆĒĢ£ ņłśņłĀņĀü ņĀłņĀ£ļź╝ ņŗ£Ē¢ēĒĢśņśĆĻ│Ā ņØ┤ņÖĆ ĒĢ©Ļ╗ś ĒĢŁĻ│Āņ¦ĆĒśłņ”ØņĀ£ņØĖ statin ņĀ£ņĀ£ļź╝ ļ│ĄņÜ®ĒĢśļÅäļĪØ ĒĢśņśĆņ£╝ļ®░ ņÖĖļל Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ņØä ĒĢśņśĆļŗż. ņ”Øņāü ļ░Å ĒÅÉņćäņä▒ ļ│æļ│ĆņØś ņ×¼ļ░£ ņåīĻ▓¼ņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░, Ļ▓░ņĀłņä▒ ļ│æļ│ĆņØś ņ¦äĒ¢ēļÅä Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż. ĒøäļæÉļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ ņāü ņä▒ļīĆņØś ņøĆņ¦üņ×ä ņĀĆĒĢś ņåīĻ▓¼ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŖöļŹ░, Ēīīņóģņä▒ ĒÖ®ņāēņóģņØ┤ Ēö╝ņŚ┤ņŚ░Ļ│©ļČĆļź╝ ņ╣©ļ▓öĒĢśņŚ¼ ĒśĖĒØĪĻ│żļ×ĆĻ│╝ ņä▒ļīĆņØś Ļ░Ćņä▒ļ¦łļ╣äĻ░Ć ļ░£ņāØĒĢ£ ņ”ØļĪĆĻ░Ć ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ņ£╝ļ®░ ņŗ¼ĒĢ£ ĒśĖĒØĪĻ│żļ×Ć ļ░Å ĻĖ░ļÅä ĒÅÉņāēņ£╝ļĪ£ ĻĖ░Ļ┤ĆņĀłĻ░£ņłĀ ļ░Å Ēö╝ņŚ┤ņŚ░Ļ│© ļé┤ņĖĪņĀłņĀ£ņłĀņØä ņŗ£Ē¢ēĒĢ£ ņé¼ļĪĆņØś ļ│┤Ļ│ĀļÅä ņ׳ņŚłĻĖ░ņŚÉ ņØ┤ņŚÉ ļīĆĒĢ┤ ļ│┤ļŗż ņŻ╝ņØśĻ╣ŖņØĆ Ļ▓ĮĻ│╝Ļ┤Ćņ░░ņØ┤ ĒĢäņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż[19].
Ēīīņóģņä▒ ĒÖ®ņāēņóģņØĆ ļ¦żņÜ░ ļō£ļ¼Ė ņ¦łĒÖśņ£╝ļĪ£ ņ”ØļĪĆņłśņØś ņĀ£ĒĢ£ņ£╝ļĪ£ ņØĖĒĢ┤ ņĢäņ¦üĻ╣īņ¦Ć ĒÖĢņŗżĒĢ£ ņ╣śļŻīļ▓ĢņØ┤ ņŚåļŗż. ĻĖ░ņĪ┤ņØś ļ¼ĖĒŚīņŚÉ ņåīĻ░£ ļÉ£ ņ╣śļŻī ļ░®ļ▓ĢļōżņØ┤ ļŗżļźĖ ĒÖśņ×ÉņŚÉĻ▓ī ĒÜ©Ļ│╝Ļ░Ć ņ׳ņØä ņ¦Ć ļ¬ģĒÖĢĒĢśĻ▓ī ļ░ØĒśĆņ¦Ćņ¦Ć ņĢŖņĢśĻĖ░ņŚÉ ņ╣śļŻī ļ░®Ē¢źņØä Ļ▓░ņĀĢĒĢśļŖöļŹ░ ņ׳ņ¢┤ ņ¢┤ļĀżņøĆņØ┤ ļö░ļźĖļŗż. ĻĘĖļ¤¼ļéś ĒÖśņ×ÉņØś ņ”ØņāüĻ│╝ ņ¦łĒÖśņØś ņŗ¼Ļ░üņä▒ņØä Ļ│ĀļĀżĒĢśņŚ¼ ņĀüņĀłĒĢ£ ĻĄŁņåīņĀü ņ╣śļŻīņÖĆ ņĀäņŗĀņĀüņØĖ ņ╣śļŻīļź╝ ļ│æĒ¢ēĒĢ£ļŗżļ®┤ ļ│┤ļŗż ņĢłņĀäĒĢśĻ│Ā ĒÜ©Ļ│╝ņĀüņØĖ ņ╣śļŻīļź╝ ĻĖ░ļīĆĒĢĀ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż.