ņä£ ļĪĀ
ņ¢æņĖĪ ņä▒ļīĆ ņÜ┤ļÅÖņןņĢĀ(bilateral vocal cord paralysis)ļŖö ņżæņČöņŗĀĻ▓ĮņØ┤ņāü, ĒøäļæÉņŗĀĻ▓ĮņØ┤ņāü, ņ£żņāüĒö╝ņŚ┤Ļ┤ĆņĀłņØś ņØ┤ņāü, Ēö╝ņŚ┤ņŚ░Ļ│©Ļ░ä Ļ│ĀņĀĢņŚÉ ņØśĒĢ┤ ļ░£ņāØĒĢśļ®░ ĒĢ┤ļŗ╣ ņØ┤ņāüņØĆ ņóģņ¢æ(tumor), ņŗĀĻ▓ĮĒĢÖņĀü ņ¦łĒÖś(neurologic disease), Ļ▓░ĒĢ®ņĪ░ņ¦üņ¦łĒÖś(connective tissue disease), ļ░śĒØöņä▒ ļ¦ØņāüņĪ░ņ¦ü(cicatrical web), ņ£żņāüĒö╝ņŚ┤Ļ┤ĆņĀł ĒāłĻĄ¼ ļō▒ņŚÉ ņØśĒĢ┤ņä£ ļ░£ņāØĒĢ£ļŗż[1,2].
Ļ▓░ĒĢ®ņĪ░ņ¦üņ¦łĒÖśņØś ĒøäļæÉ ņ╣©ļ▓öņØĆ ņ¢æņĖĪ ņä▒ļīĆ ņÜ┤ļÅÖņןņĢĀņØś ņøÉņØĖņ£╝ļĪ£ļŖö ĒØöĒĢśņ¦Ć ņĢŖņ£╝ļéś ĒÖ£ļÅÖņä▒ Ļ▓░ĒĢ®ņĪ░ņ¦üņ¦łĒÖśņØä Ļ░Ćņ¦ä ĒÖśņ×ÉņŚÉņä£ļŖö 30%ņŚÉņä£ ņ£żņāüĒö╝ņŚ┤Ļ┤ĆņĀł ņ╣©ļ▓öņØ┤ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż[3]. ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņØĆ 31% ņØ┤ņāüņŚÉņä£ ĒøäļæÉĻ┤ĆņĀłņØä ņ╣©ļ▓öĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłņ£╝ļ®░ ņ¦üņĀæ Ļ┤ĆņĀł ņ╣©ļ▓ö ņÖĖņŚÉļÅä ĒśłĻ┤ĆņŚ╝(vasculitis)ņŚÉ ņØśĒĢ£ ĒøäļæÉņŗĀĻ▓Į ļ░Å ļ»ĖņŻ╝ņŗĀĻ▓ĮņØś ņŗĀĻ▓Įļ│æņ”Ø, ņŚ╝ņ”Øņä▒ ņ£ĪņĢäņĪ░ņ¦üņ£╝ļĪ£ ņØĖĒĢ£ ņĢĢļ░Ģ ļō▒ņŚÉ ņØśĒĢ┤ ņä▒ļīĆ ņÜ┤ļÅÖņןņĢĀļź╝ ņØ╝ņ£╝Ēé¼ ņłś ņ׳ļŗż[4,5]. ņØ┤ ņżæ Ļ░Ćņן ļ¦ÄņØ┤ ļ░£ņāØĒĢśļŖö ņøÉņØĖņØĆ ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņØś ņ£żņāüĒö╝ņŚ┤Ļ┤ĆņĀł ņ╣©ļ▓öņØ┤Ļ│Ā ņØ┤ļŖö ĻĄŁļé┤ņŚÉļÅä ļ¬ć ņ░©ļĪĆ ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ņ£╝ļéś[6,7], ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņŚÉņä£ ĒøäļæÉ ņŗĀĻ▓Į ļ░Å ļ»ĖņŻ╝ņŗĀĻ▓ĮņØś ņŗĀĻ▓Įļ│æņ”ØņØä ļÅÖņŗ£ņŚÉ ļ│┤ņØĖ ņ¢æņĖĪ ņä▒ļīĆļ¦łļ╣äļŖö ĻĄŁļé┤ņŚÉņä£ļŖö ņĢäņ¦ü ļ│┤Ļ│ĀļÉ£ ņśłĻ░Ć ņŚåļŗż. ņĀĆņ×ÉļōżņØĆ ĒøäļæÉ ņŗĀĻ▓ĮĻ│╝ ņ£żņāüĒö╝ņŚ┤ Ļ┤ĆņĀłņØś ņ╣©ļ▓öņØä ļÅÖņŗ£ņŚÉ ļ│┤ņØ┤ļŖö ņ¢æņĖĪ ņä▒ļīĆ ļ¦łļ╣ä 1ņśłļź╝ Ļ▓ĮĒŚśĒĢśņśĆņ£╝ļ®░ ņØ┤ļź╝ ļ│┤Ļ│ĀĒĢśļŖö ļ░öņØ┤ļŗż.
ņ”Ø ļĪĆ
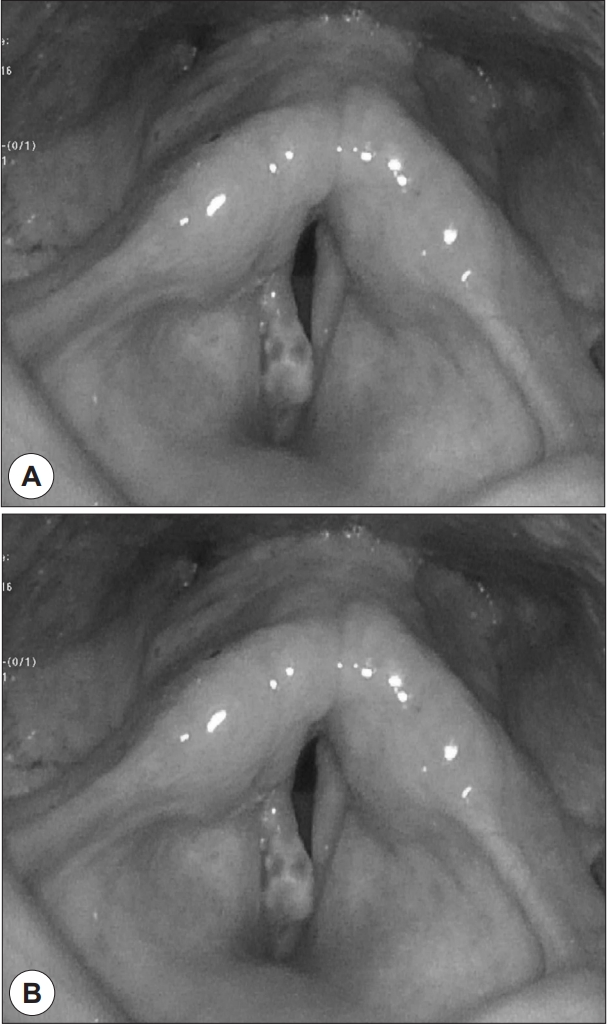
64ņäĖ ļé©ņ×É ĒÖśņ×ÉĻ░Ć 4Ļ░£ņøö ņĀäļČĆĒä░ ņŗ£ņ×æļÉ£ ĒśĖĒØĪĻ│żļ×ĆņØä ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢśņśĆļŗż. ĒśĖĒØĪĻ│żļ×Ć ņØ┤ņÖĖņŚÉ ņē░ļ¬®ņåīļ”¼ļź╝ ĒśĖņåīĒĢśņśĆņ£╝ļ®░ ĒĢ┤ļŗ╣ ņ”ØņāüņØĆ 1ļģä ņØ┤ņāü ņ¦ĆņåŹļÉśņŚłļŗż. Ļ│ĀĒśłņĢĢ ņÖĖņŚÉļŖö ņ¦äļŗ©ļ░øņØĆ ņ¦łĒÖś ņŚåņŚłņ£╝ļ®░ ņŻ╝ 3ĒÜīņØś ņØīņŻ╝ļĀźĻ│╝ 20Ļ░æļģäņØś ĒØĪņŚ░ļĀźņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ņŚłļŗż. ĒÖśņ×ÉļŖö 5ļģä ņĀäļČĆĒä░ ņÜ░ņĖĪ ļŗżļ”¼ļź╝ ņĀłņŚłņ£╝ļ®░(limping gait) 2ļģä ņĀäļČĆĒä░ ņ¢æņåÉ ļ¢©ļ”╝Ļ│╝(both hands intension tremor)Ļ│╝ ņłśļ®┤ ņżæ ņÜ┤ļÅÖņןņĢĀļź╝ ĒśĖņåīĒĢśĻ│Ā ņ׳ņŚłļŗż. ĒøäļæÉļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ ņåīĻ▓¼ņŚÉņä£ ņóīņĖĪ ņä▒ļīĆņØś ņÖäņĀäļ¦łļ╣ä, ņÜ░ņĖĪ ņä▒ļīĆņØś ļČłņÖäņĀäļ¦łļ╣ä ņåīĻ▓¼Ļ│╝ ĒĢ©Ļ╗ś ņÜ░ņĖĪ ņä▒ļīĆņŚÉ ņÜ®ņóģņØ┤ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░(Fig. 1), ļæÉĻ▓ĮļČĆ ņØ┤ĒĢÖņĀü Ļ▓Ćņé¼ ņāü ļŗżļźĖ ĒŖ╣ņØ┤ ņåīĻ▓¼ņØĆ ņŚåņŚłļŗż. ņ▓£ļ¬ģ ļ░Å ĒśĖĒØĪĻ│żļ×Ć ņ”Øņāü ņŗ¼ĒĢśņŚ¼ ļé┤ņøÉ ļŗ╣ņØ╝ ņØæĻĖē ĻĖ░Ļ┤ĆņĀłĻ░£ņłĀņØä ņŗ£Ē¢ēĒĢśņśĆļŗż.
ņ¢æņĖĪ ņä▒ļīĆļ¦łļ╣ä ņøÉņØĖĻ░Éļ│äņØä ņ£äĒĢ┤ ĒśłņĢĪĻ▓Ćņé¼, ĒøäļæÉĻĘ╝ņĀäļÅä(laryngeal electromyography), Ļ▓ĮļČĆņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśü, ļćī ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāüņ┤¼ņśü, ĒøäļæÉļ»ĖņäĖņłśņłĀ(laryngomicrosurgery)ņØä ņŗ£Ē¢ēĒĢśņśĆļŗż. ĒøäļæÉĻĘ╝ņĀäļÅä(laryngeal electromyography)ņāü ņ¢æņĖĪ ņāüĒøäļæÉņŗĀĻ▓Į(superior laryngeal nerve)Ļ│╝ ļÉśļÅīņØ┤ĒøäļæÉņŗĀĻ▓Į(recurrent laryngeal nerve) ļ¬©ļæÉņŚÉņä£ ļČłņÖäņĀäĒĢ£ Ļ░äņäŁņ¢æņāüņØä ļ│┤ņśĆņ£╝ļ®░ ņóīņĖĪ ļÉśļÅīņØ┤ĒøäļæÉņŗĀĻ▓ĮņŚÉņä£ ņ¢æņä▒ņśłĒīīĻ░Ć Ļ┤Ćņ░░ļÉśņŚłļŗż. ļćī MRIņāü ĒŖ╣ņØ┤ ņåīĻ▓¼ ņŚåņŚłņ£╝ļ®░, ņŗĀĻ▓ĮņĀäļÅäĻ▓Ćņé¼(Sensory-motor nerve conduction study), FĒīī Ļ▓Ćņé¼(F wave study), H ļ░śņé¼ Ļ▓Ćņé¼(H reflex study), ļćīĒīīĻ▓Ćņé¼ (Electroencephalogram) ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░ ņĀĢņāüņåīĻ▓¼ ļ│┤ņŚ¼ ļŗżļźĖ ņŗĀĻ▓ĮĒĢÖņĀü ļ│æļ│ĆņØĆ ņŚåļŖö Ļ▓āņ£╝ļĪ£ ĒīÉļ¬ģļÉśņŚłļŗż. ļö░ļØ╝ņä£ ĒøäļæÉĻĘ╝ņĀäļÅäņŚÉņä£ ņ¦äļŗ©ļÉ£ ņ¢æņĖĪ ņāüĒøäļæÉņŗĀĻ▓Į ļ░Å ļÉśļÅīņØ┤ĒøäļæÉņŗĀĻ▓ĮņØś ņŗĀĻ▓Įļ│æņ”ØņØĆ RAņŚÉ ņØśĒĢ£ ņ¢æņĖĪ ļ»ĖņŻ╝ņŗĀĻ▓Į(vagus nerve) ļ│æņ”ØņŚÉ ņØśĒĢ£ Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉśņŚłļŗż.
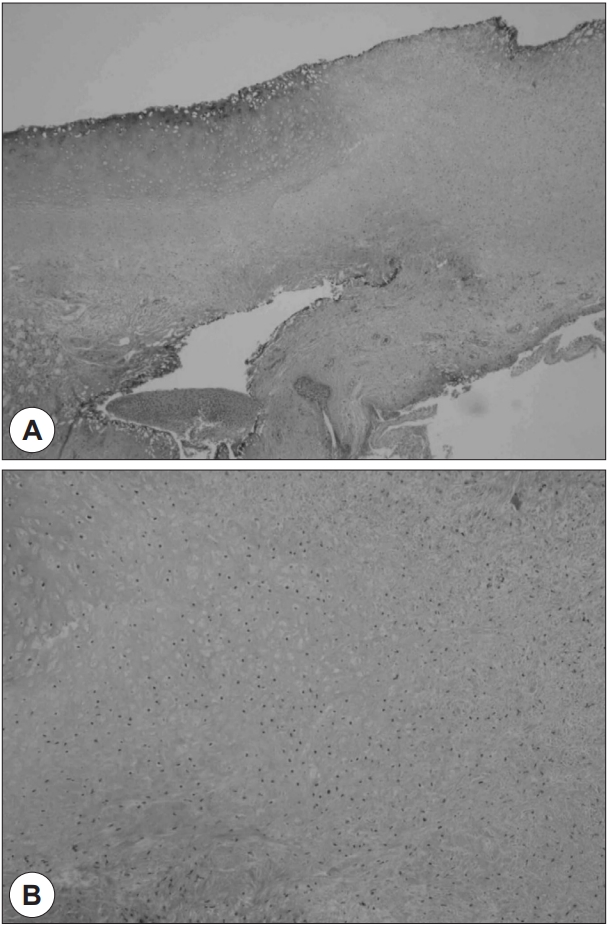
Ļ▓ĮļČĆņĀäņé░ĒÖö ļŗ©ņĖĄņ┤¼ņśüņāüņŚÉņä£ ņÜ░ņĖĪ ņä▒ļīĆņŚÉ 7 mm Ēü¼ĻĖ░ņØś ņÜ®ņóģ ņØ┤ņÖĖņØś ĒŖ╣ņØ┤ņé¼ĒĢŁņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░ ņÜ®ņóģ ņĀ£Ļ▒░ ļ░Å ĻĖ░ļÅä ĒÖĢļ│┤, Ļ┤ĆņĀłļČĆņ£ä ņ┤ēņ¦ä ļ░Å ņāØĻ▓Ćļź╝ ņ£äĒĢ┤ ĒśäņłśĒøäļæÉĻ▓ĮĻ│╝ ņłśņłĀĒśäļ»ĖĻ▓ĮņØä ņØ┤ņÜ®ĒĢśņŚ¼ ĒøäļæÉļ»ĖņäĖņłśņłĀ(laryngomicrosurgery)ņØä ņŗ£Ē¢ēĒĢśņśĆļŗż. ļ»ĖņäĖņłśņłĀĻĖ░ĻĄ¼ļź╝ ņØ┤ņÜ®ĒĢ£ Ēö╝ņŚ┤ņŚ░Ļ│©ņ┤ēņ¦äņŚÉņä£ ņóīņĖĪ ņ£żņāüĒö╝ņŚ┤Ļ┤ĆņĀłņØś ņøĆņ¦üņ×ä ņĀĆĒĢśĻ░Ć Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░ ņÜ░ņĖĪ ņ£żņāüĒö╝ņŚ┤Ļ┤ĆņĀłņØś ņøĆņ¦üņ×äņØĆ ņĀĢņāüņØ┤ņŚłļŗż. ņÜ░ņĖĪ ņÜ®ņóģņØä ņĀ£Ļ▒░ĒĢśņśĆņ£╝ļ®░ ĻĖ░ļÅä ĒÖĢļ│┤ ļ░Å ņĪ░ņ¦ü ņāØĻ▓ĆņØś ļ¬®ņĀüņ£╝ļĪ£ ņóīņĖĪ ļĀłņØ┤ņĀĆ Ēøäļ░® ņä▒ļīĆņĀłņĀ£ņłĀ(LASER posterior cordectomy)ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņłĀ Ēøä 3ņØ╝ ņ¦Ė ĒśĖĒØĪ ņĢłņĀĢļÉśņ¢┤ ĻĖ░Ļ┤ĆĒŖ£ļĖī ņĀ£Ļ▒░ĒĢśņśĆļŗż. ņłĀ Ēøä ņĪ░ņ¦üļ│æļ”¼Ļ▓Ćņé¼ Ļ▓░Ļ│╝ņŚÉņä£ ņóīņĖĪ ņ£żņāüĒö╝ņŚ┤ņŚ░Ļ│© ņŻ╝ļ│Ć ņĪ░ņ¦üņØś ņŚ░Ļ│©ņŚ╝(perichondritis) ņåīĻ▓¼ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 2). ļźśļ¦łĒŗ░ņŖż ļé┤Ļ│╝ Ēśæņ¦ä ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░ ĒśłņĢĪĻ▓Ćņé¼ņāü ļźśļ¦łĒŗ░ņŖż ņØĖņ×É(rheumatoid factor, RF) 87 IU/mL, ņĀüĒśłĻĄ¼ ņ╣©Ļ░ĢņåŹļÅä(ESR) 43 mm/hr, ņĀĢļ¤ēņĀüC reactive protein(CRP) 4.48 mg/dLļĪ£ ņ”ØĻ░ĆļÉ£ ņåīĻ▓¼ ļ│┤ņśĆņ£╝ļ®░ anti cyclic citrullinated peptide(ĒĢŁCCP) ĒĢŁņ▓┤ ņ¢æņä▒ņØ┤ņŚłļŗż. ņ┤¼ņśüĒĢ£ ņłśļČĆ ļ░®ņé¼ņäĀ Ļ▓Ćņé¼ņŚÉņä£ ņåÉĻ│╝ ļ░£ņØś ļŗżļ░£ņä▒ Ļ│© ļ»Ėļ×Ć(multiple bony erosion)ņØ┤ Ļ┤Ćņ░░ļÉśņ¢┤ ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ ņ¦äļŗ© ĻĖ░ņżĆņŚÉ ļČĆĒĢ®ĒĢśņŚ¼ ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņ£╝ļĪ£ ņ¦äļŗ©ļÉśņŚłļŗż(Fig. 3).
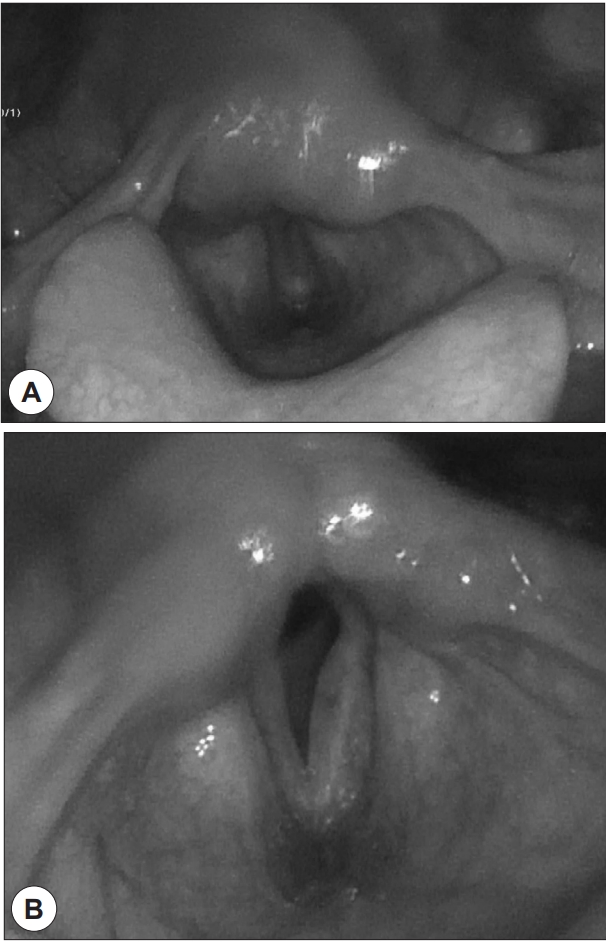
ĒÖśņ×É sulfasalazine 500 mg ĒĢśļŻ© 2ĒÜī, methotrexate 20 mg ņŻ╝ 1ĒÜī, corticosteroid 15 mg ĒĢśļŻ© 1ĒÜī ļ│ĄņÜ®ĒĢśņśĆņ£╝ļ®░ Ēł¼ņĢĮ 3Ļ░£ņøö Ēøä ņŗ£Ē¢ēĒĢ£ ĒøäļæÉ ļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ņāü ņóīņĖĪ ņä▒ļīĆ ņøĆņ¦üņ×ä ĒÜīļ│ĄņØä ĒÖĢņØĖĒĢśņśĆļŗż(Fig. 4).
Ļ│Ā ņ░░
ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņØś ĒøäļæÉ ņ╣©ļ▓öņØĆ 1880ļģäļÅäņŚÉ Morell MacKenzie ņ▓śņØīņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż[8]. ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņØś ĒøäļæÉ ņ╣©ļ▓ö ņ£Āļ│æļźĀņØĆ ļé©ņä▒ļ│┤ļŗż ņŚ¼ņä▒ņŚÉņä£ ļŹö ļåÆĻ│Ā[9] ĒøäļæÉĻ▓ĮņāüņŚÉņä£ Ļ┤Ćņ░░ļÉśļŖö ĒøäļæÉņØś ņ╣©ļ▓öņØĆ ņĢĮ 30~70%, CTņŚÉņä£ Ļ┤Ćņ░░ļÉśļŖö ņ£Āļ│æļźĀņØĆ ņĢĮ 50~70%ņØ┤ļŗż[10]. ļīĆļČĆļČä ņ”ØņāüņØ┤ ņŚåņ£╝ļ®░ ņĢĮ 26%ļ¦īņØ┤ ņ”ØņāüņØä ĒśĖņåīĒĢ£ļŗż[11]. ĒøäļæÉ ņ╣©ļ▓öņŗ£ ņ┤łĻĖ░ ņ”ØņāüņØĆ ļ¬®ņØś ņØ┤ļ¼╝Ļ░Éņ£╝ļĪ£ ļéśĒāĆļéś Ļ░äĻ│╝ĒĢśĻĖ░Ļ░Ć ņēĮļŗż. ļ│æļ│ĆņØ┤ ņ¦äĒ¢ēļÉĀ Ļ▓ĮņÜ░ ņĢĀņä▒, ĻĖ░ņ╣©, ņŚ░ĒĢśĻ│żļ×Ć ļō▒ņØś ņ”ØņāüņØ┤ ļéśĒāĆļéśļ®░ ņŗ¼ĒĢĀ Ļ▓ĮņÜ░ ĒśĖĒØĪĻ│żļ×ĆņØä ņØ╝ņ£╝ņ╝£ ĒĢ┤ļŗ╣ Ļ▓ĮņÜ░ņŚÉļŖö ņØæĻĖē ĻĖ░Ļ┤ĆņĀłĻ░£ņłĀņØ┤ ĒĢäņÜöĒĢśļŗż[11].
ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņŚÉņä£ ņä▒ļīĆ ļ¦łļ╣äļź╝ ņ£Āļ░£ĒĢśļŖö ļ│æĒā£ņāØļ”¼ļĪ£ļŖö ņ£żņāüĒö╝ņŚ┤Ļ┤ĆņĀłņØś ĒÖ£ņĢĪļ¦ē(synovium)ņØś ņŚ╝ņ”Øņ£╝ļĪ£ ņØĖĒĢ£ Ļ┤ĆņĀłļ®┤ņØś ņä¼ņ£ĀĒÖö, ļźśļ¦łĒŗ░ņŖż Ļ▓░ņĀłļĪ£ ņØĖĒĢ£ ņä▒ļīĆĻĘ╝(vocalis muscle)ņØ┤ļéś ņ£żņāüĒö╝ņŚ┤ Ļ┤ĆņĀłņØś ņøĆņ¦üņ×ä ņןņĢĀ. ĒśłĻ┤ĆņŚ╝ ļ░Å ĒøäļæÉ ļÉśļÅīņØ┤ ņŗĀĻ▓ĮĻ│╝ ļ»ĖņŻ╝ ņŗĀĻ▓ĮņØś Ēć┤ĒÖöļĪ£ ņØĖĒĢ£ ņŗĀĻ▓Įļ│æņ”Ø, Ļ▓ĮņČöļ╝ł(cervical spine)ņØś ļźśļ¦łĒŗ░ņŖż ņ╣©ļ▓öņ£╝ļĪ£ ņØĖĒĢ┤ Ļ▓ĮņłśņŚ░ņłś ņĢĢļ░Ģ(cervicomedullary compression) ļō▒ņØ┤ ļ│┤Ļ│ĀļÉśņŚłļŗż[11]. ņ╣śļŻīļŖö ņŖżĒģīļĪ£ņØ┤ļō£, ļ╣äņŖżĒģīļĪ£ņØ┤ļō£ ĒĢŁņŚ╝ņĀ£(nonsteroid anti-inflammatory), ĒĢŁļźśļ¦łĒŗ░ņŖż ņĢĮļ¼╝ ņ╣śļŻīĻ░Ć ņ׳ņ£╝ļ®░ ņ¢æņĖĪ ņä▒ļīĆļ¦łļ╣äĻ░Ć ļ░£ņāØĒĢ£ Ļ▓ĮņÜ░ņŚÉļŖö ņŖżĒģīļĪ£ņØ┤ļō£ Ēł¼ņŚ¼Ļ░Ć ņÜ░ņäĀņĀü ņ╣śļŻīņØ┤ļ®░ Ēł¼ņŚ¼ļ░®ļ▓Ģņ£╝ļĪ£ļŖö ņĀäņŗĀņĀü Ēł¼ņŚ¼ņÖĆ ĻĄŁņåī Ļ┤ĆņĀłņŻ╝ņé¼ļź╝ ņŗ£Ē¢ēĒĢ┤ ļ│╝ ņłś ņ׳ļŗż[12]. ĒÖ£ļÅÖņä▒ Ļ┤ĆņĀłņŚ╝ņØś ņ¦äĒ¢ēņØä ļ¦ēļŖöļŹ░ ņé¼ņÜ®ļÉśļŖö methotrexateļŖö ļŗ©ļÅģņÜ®ļ▓ĢņØ┤ļéś ļ│æĒĢ®ņÜöļ▓Ģņ£╝ļĪ£ ņé¼ņÜ®ļÉ£ļŗż[13].
ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņŚÉ ņØśĒĢ£ ņ¢æņĖĪ ņä▒ļīĆļ¦łļ╣äļŖö ņŻ╝ļĪ£ ņ£żņāüĒö╝ņŚ┤Ļ┤ĆņĀłņØś ņ╣©ļ▓öņ£╝ļĪ£ ļ░£ņāØĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äņ£╝ļéś, ļ│Ė ņ”ØļĪĆņŚÉņä£ļŖö ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņØä ņ¦äļŗ© ļ░øĻĖ░ ņĀä ĒśĖĒØĪĻ│żļ×ĆņØä ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢśņśĆņ£╝ļ®░ ņØ┤Ēøä ņŗ£Ē¢ēĒĢ£ ĒøäļæÉĻĘ╝ņĀäļÅäļź╝ ĒåĄĒĢ┤ ņŗĀĻ▓Įļ│æņ”ØņØ┤ ņ¦äļŗ©ļÉśņŚłņ£╝ļ®░ ņĪ░ņ¦üĻ▓Ćņé¼ļź╝ ĒåĄĒĢ┤ Ēö╝ņŚ┤ņŚ░Ļ│©ļ¦ēņØś ņŚ╝ņ”ØņåīĻ▓¼ņØä ĒÖĢņØĖ ĒĢ©ņ£╝ļĪ£ņŹ©, ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņŚÉ ņØśĒĢ£ ļ»ĖņŻ╝ņŗĀĻ▓ĮņŚ╝Ļ│╝ ņ£żņāüĒö╝ņŚ░Ļ┤ĆņĀłņØś Ļ│ĀņĀĢņØ┤ ļÅÖņŗ£ņŚÉ ļ░£ņāØĒĢśņŚ¼ Ļ▓░Ļ│╝ņĀüņ£╝ļĪ£ ņ¢æņĖĪņä▒ļīĆļ¦łļ╣äĻ░Ć ļéśĒāĆļé£ Ļ▓āņ£╝ļĪ£ ĒīÉļŗ©ĒĢĀ ņłś ņ׳ņŚłļŗż. ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ņØś ņŗĀĻ▓Įļ│æņ”Ø ņ£Āļ░£ļĪ£ ņØĖĒĢ£ ņ¢æņĖĪ ņä▒ļīĆļ¦łļ╣äļŖö 1958ļģä Darkeļō▒ņŚÉ ņØśĒĢ┤ ļ│┤Ļ│ĀļÉśņŚłņ£╝ļéś ņØ┤ļŖö ņé¼Ēøä ļČĆĻ▓Ćņ£╝ļĪ£ ņŗĀĻ▓ĮņØś Ēāłņłśņ┤łĒÖö ņåīĻ▓¼ņØä ļ░£Ļ▓¼ĒĢśņśĆņ£╝ļ®░ ņ×äņāüņĀüņ£╝ļĪ£ ņŗĀĻ▓Įļ│æņ”ØņØä ņ¦äļŗ©ĒĢ£ ņé¼ļĪĆļ│┤Ļ│ĀļŖö Ēśäņ×¼Ļ╣īņ¦Ć ņŚåļŗż[14]. ņä▒ļīĆļ¦łļ╣äĒÖśņ×ÉņŚÉņä£ ĒøäļæÉĻĘ╝ņĀäļÅäļŖö Ļ┤ĆņĀł ņןņĢĀļĪ£ ņØĖĒĢ£ ņä▒ļīĆņØś Ļ│ĀņĀĢ(fixation)Ļ│╝ ņŗĀĻ▓Įļ│æņ”ØņØś Ļ░Éļ│äņŚÉ ļÅäņøĆņØä ņżä ņłś ņ׳ļŗż[15]. ņ¢æņĖĪ ņä▒ļīĆļ¦łļ╣ä ĒÖśņ×ÉņŚÉņä£ ĒøäļæÉĻĘ╝ņĀäļÅäņØś ņŗ£Ē¢ēņØĆ ņä▒ļīĆļČĆņóģ, ņČ£Ēśł ļō▒ņ£╝ļĪ£ ĒśĖĒØĪĻ│żļ×ĆņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ņ¢┤ ĻĖ░ļÅä ĒÖĢļ│┤ Ēøä Ļ▓Ćņé¼ņŗ£Ē¢ēņØä Ļ│ĀļĀżĒĢĀ ņłś ņ׳ņ£╝ļ®░, ļ│Ė ņ”ØļĀłņŚÉņä£ļŖö ĻĖ░Ļ┤ĆņĀłĻ░£ņłĀ Ēøä ņāüĒā£ļĪ£ ĒøäļæÉĻĘ╝ņĀäļÅäļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņ¢æņĖĪ ĒøäļæÉ ņŗĀĻ▓Į ļ¬©ļæÉ ņŗĀĻ▓ĮņĀÉņ”ØņØ┤ ĻĖēĻ▓®Ē׳ Ļ░ÉņåīļÉśņ¢┤ņ׳Ļ│Ā ņ¢æņä▒ņśłĒīīņØś ļ░£ĒśäņØ┤ ņŗĀĻ▓ĮĻ│╝ ņĀäļ¼ĖņØśņŚÉ ņØśĒĢ┤ ĒÖĢņØĖļÉśņ¢┤ ņ¢æņĖĪ ĒøäļæÉņŗĀĻ▓Įļ│æņ”Øņ£╝ļĪ£ ņ¦äļŗ©ĒĢśņśĆņ£╝ļéś ņĪ░ņ¦üĻ▓Ćņé¼ Ļ▓░Ļ│╝ņŚÉņä£ ļźśļ¦łĒŗ░ņŖżĻ┤ĆņĀłņŚ╝ņØś Ļ┤ĆņĀłņ╣©ļ▓öņØ┤ ņ¦äļŗ©ļÉśņŚłļŗż. ņ¢æņĖĪņä▒ ņä▒ļīĆļ¦łļ╣ä ĒÖśņ×ÉņŚÉņä£ļŖö ļ│Ė ņ”ØļĪĆņÖĆ Ļ░ÖņØĆ ļźśļ¦łĒŗ░ņŖż Ļ┤ĆņĀłņŚ╝ ļō▒ Ļ▓░ņ▓┤ņĪ░ņ¦üņ¦łĒÖśņØś Ļ┤ĆņĀł ņ╣©ļ▓ö ļ░Å ĒĢ┤ļŗ╣ ņ¦łĒÖśņØś ņŗĀĻ▓Įļ│æņ”Ø ņ£Āļ░£Ļ░ĆļŖźņä▒ņØä ļ░░ņĀ£ĒĢśņ¦Ć ņĢŖĻ│Ā ņ▓ĀņĀĆĒĢ£ ļ│æļĀź ņ▓ŁņĘ©ņÖĆ ĒāĆĻ│╝ Ēśæņ¦äņØä ĒåĄĒĢ£ ņ¦äļŗ© ļģĖļĀźņØ┤ ĒĢäņÜöĒĢśļŗż.