갑상선 수술 후 발생하는 음성장애의 치료
Abstract
Hoarseness is a postoperative complication of thyroidectomy, mostly due to damage to the recurrent laryngeal nerve (RLN). Hoarseness may also be brought about via vocal cord dysfunction (VCD) due to injury of the vocal cords from manipulations during anesthesia, as well as from psychogenic disorders and respiratory and upper-GI related infections. The clinician or surgeon should 1) document assessment of the patient’s voice once a decision has been made to proceed with thyroid surgery ; 2) examine vocal fold mobility, or refer the patient to a clinician who can examine vocal fold mobility 3) examine vocal fold mobility, or refer the patient to a clinician who can examine vocal fold mobility, once a decision has been made to proceed with thyroid surgery 4) educate the patient about the potential impact of thyroid surgery on voice once a decision has been made to proceed with thyroid surgery ; 5) inform the anesthesiologist of the results of abnormal preoperative laryngeal assessment in patients who have had laryngoscopy prior to thyroid surgery ; 6) take steps to preserve the external branch of the surperior laryngeal nerve(s) when performing thyroid surgery ; 7) document whether there has been a change in voice between 2 weeks and 2 months following thyroid surgery ; 8) examine vocal fold mobility or refer the patient for examination of vocal fold mobility in patients with a change in voice following thyroid surgery ; 9) refer a patient to an otolaryngologist when abnormal vocal fold mobility is identified after thyroid surgery ; 10) counsel patients with voice change or abnormal vocal fold mobility after thyroid surgery on options for voice rehabilitation.
Key words: Dysphonia; Thyroidectomy; Laryngeal nerve
중심 단어: 음성장애; 갑상선절제술; 반회후두신경; 상후두신경; 갑상선 수술 후 증후군
서 론
갑상선 수술 후 발생하는 음성장애는 비교적 흔하게 경험하는 질환이다[ 1]. 갑상선을 수술하는 외과의의 관점에서 성대마비가 없는 음성장애에 대하여 정확한 원인을 찾기 어렵고, 일시적인 경우도 많아 환자는 불편감을 호소하나 의사로서 특별히 해줄것이 없는 대표적 질환중 하나로 인식되어 왔다. 최근 미국 가이드라인에서 정리한 대표적인 원인분류로는 1) 반회두두신경 손상 2) 상후두신경의 외분지 손상 3) 윤상갑상근의 직접적 손상 4) 연부조직 손상 5) 기관삽관과 관련된 손상 6) 상기도감염등의 원인등으로 분류하였다( Table 1) [ 2].
본 론
1. 갑상선의 수술적 해부학 구조 및 수술 분류
갑상선 수술시 수술 후 음성변화와 관련되어 가장 중요한 것은 1) 반회후두신경 2) 상후두신경의 외분지라 하겠다. 물론, 윤상갑상근 및 피대근 strap muscle 등 역시 수술 후 섬유화등의 원인으로 수술 후 음성변화에 영향을 주지만 외과적 관점에서 가장 중요한 것은 위의 두가지 신경이다. 최근 갑상선 암 치료지침의 많은 변화가 있어 적절한 수술 범위등이 재확립되고 있으나, 기본적으로 예후인자등에 따라 갑상선의 수술범위가 달라지며 임파선 전이여부에 따라 주변 임파선 제거의 범위 역시 달라지므로 어떤 수술을 시행했느냐에 따라 다른 결과가 생길 수 있음 역시 주지하여야 하겠다.
반회후두신경은 암침범이 없는 한 대부분 보존되지만, 환자에 따라 신경이 얇고 특히 신경이 후두로 들어가는 부위의 berry’s ligament 부위에서는 일시적 마비가 발생할 위험이 있다. 상후두신경의 외분지는 대부분의 갑상선 수술중 적극적으로 확인하지는 않지만 갑상선 피막에 붙여서 수술을 진행하기 때문에 손상의 우려가 높지는 않지만 그림에서와 같이 외분지가 갑상선 상극 하부에서 분지되는 경우 의도치 않은 손상의 가능성이 있다( Fig. 1). 갑상선 수술은 수술의 목적과 병변의 정도, 환자의 미용적 요구등에 따라 최근에는 고전적인 절개방법을 통한 수술은 물론이고 액와부 transaxillary 혹은 후이개 retroauricular approach 접근법 등을 통한 내시경하 혹은 로봇수술 등이 활발하게 시행되고 있다. 수술범위에 따라 갑상선 전절제 및 일엽절제등으로 나뉘어 진다. 보고에 따르면 대체로 내시경과 로봇수술은 고전적 절개에 의한 수술방법에 비하여 장기적으로 음성 변화 빈도에 차이가 없는 것으로 보고되나[ 3] 기본적으로 수술을 위한 작업공간이 크기 때문에 모든 환자에서 적용되는 내용은 아닐 수 있겠다. 최근에는 갑상선 수술시 이러한 반회후두신경과 상후두신경의 외분지 보존을 위한 신경 감시를 시행하는 경우가 많고, 특히 재수술이나 진행된 암의 경우 적극적으로 이를 시행하여 신경손상의 빈도를 줄이고 있다.
2. 수술전후 음성검사
의료 환경이 전혀 다른 상황이므로 국내에서 그대로 적용이 가능한가 하는 의문은 있으나, 최근의 미국 가이드라인에 따르면 baseline voice assessment를 모든 환자에서 시행하는 것을 권고하고 있다[ 2]. 또한, 모든 환자에서 후두내시경 혹은 stroboscope을 이용한 성대움직임에 대한 기록이 필효하며 이러한 성대움직임을 확인하기 어려운 환경이라면 가능한 곳으로 의뢰하여 확인하기를 권고하고 있다. 마찬가지로 수술 후 2주에서 2달 사이 성대움직임에 대한 관찰과 음성검사 역시 권고사항이다[ 2].
3. 수술전후 환자와의 상담
수술전 환자에게 목소리 이상여부를 확인하며, 수술 후 발생할 수 있는 신경손상과 음성변화 가능성에 대하여 설명하고 수술 후 목소리 변화 혹은 exercise tolerance 감소, 혹은 vocal effort의 증가 등의 현상이 2주 이상 지속되면 반드시 담당의료진에 알릴것과 음성변화가 발생하여도 이를 교정할 수 있는 여러가지 있다는 사실을 상담하여야 한다[ 2]. 수술 후 목소리가 변하였다면, 환자에게 성대마비의 가능성을 설명하고 이러한 증상이 수개월 이상 지속될 수도 있음을 혹은 회복되지 않을 수 있음 역시 설명하며 수술적 방법부터 음성치료까지 여러 치료방법이 있음을 설명한다.
4. 갑상선 수술 후 발생한 성대마비의 치료
갑상선 수술 후 발생한 일측성 성대마비의 치료로 가이드라인에서 정리한 방법은 표와 같다( Table 2) [ 2]. 임상에서 가장 손쉽게 시행할 수 있는 방법은 성대내 주입술인데, 통상적으로 외래에서 매우 빠른 시간안에 환자의 큰 불편없이 음성을 개선시킬 수 있는 유용한 시술이다. 일반적 성대내 주입술에 비하여 갑상선 수술 후 발생한 경우는 주사부위의 섬유화로 주사부위의 정확한 위치확인이 어려운 경우가 종종 있어 시술이 만족스럽게 되지 않을 수 있으며 주입물질은 대부분 영구적 물질이 아니어서 시간이 지남에 따라 흡수되고 필요시 재주사 혹은 영구마비시 외부절개를 통한 갑상성형술 thyroplasty 등이 필요할 수 있음을 환자에게 고지하여야 한다. 이외에도 수술중 신경의 희생이 명확한 경우 주변 ansa cervicalis와 recurrent laryngeal nerve의 단단문합을 통하여 vocal fold position과 bulk를 보존하는데 도움을 줄 수 있다. 음성치료는 비침습적으로 환자에 도움을 줄 수 있는 방법이며 위와 같은 여러 치료 방법중 가장 적절한 것을 적절한 시점에 시행하는 것이 필요하다. 상후두신경의 외분지 마비의 가장 큰 문제는 마비여부를 정확히 진단하기가 어렵다는 점이다. 환자의 증상 역시 애매하여 vocal fatigue, pitch 상승의 어려움등을 호소하며 후두내시경과 후두근전도에서 역시 명확한 진단이 어렵다. 상후두신경 손상 이외에도 윤상갑상근의 직접적인 손상이나 연부조직의 섬유화 등 역시 동일한 증상을 보일 수 있다. 환자의 증상에 맞추어 음성치료등을 시행하며 제4형 갑상성형술의 방법으로 치료하였다는 보고는 있으나 보편적으로 시행되지 않는다.
5. Post-Thyroidectomy Syndrome
전술한 원인 이외에 명확한 원인을 찾을 수 없으나 비특이적인 음성 및 연하장애를 호소하는 경우를 종종 볼수 있다. 수술은 문제 없이 끝났으나 어떻게 된 일인지 수술 부위가 시멘트를 발라놓은 것 같이 단단하고 당기고 조이고 막히고 목이 쉽게 피로해지고 말을 오래하면 목소리 톤이 낮아지고 쉰목소리가 나는 등의 다양한 증상을 호소하는 것이 보통이다. 여러가지 원인이 가능하겠으나 기관삽관의 영향, strap muscle fixation, laryngeal venous drainge의 변화, 수술후 갑상선 호르몬 circadian level의 불균형등 많은 원인이 제기되고 있다[ 4].
결 론
갑상선 수술 후 발생하는 음성변화의 원인은 다양하며 수술 전 후의 평가와 상담, 음성변화가 발생한 경우 최적의 치료 및 재활이 이루어 질 수 있도록 외과의와 언어치료사, 환자와 가족 모두의 유기적 협조가 필수적이다.
Figure 1.
반회후두신경 및 상후두신경 외분지의 해부학적 주행. 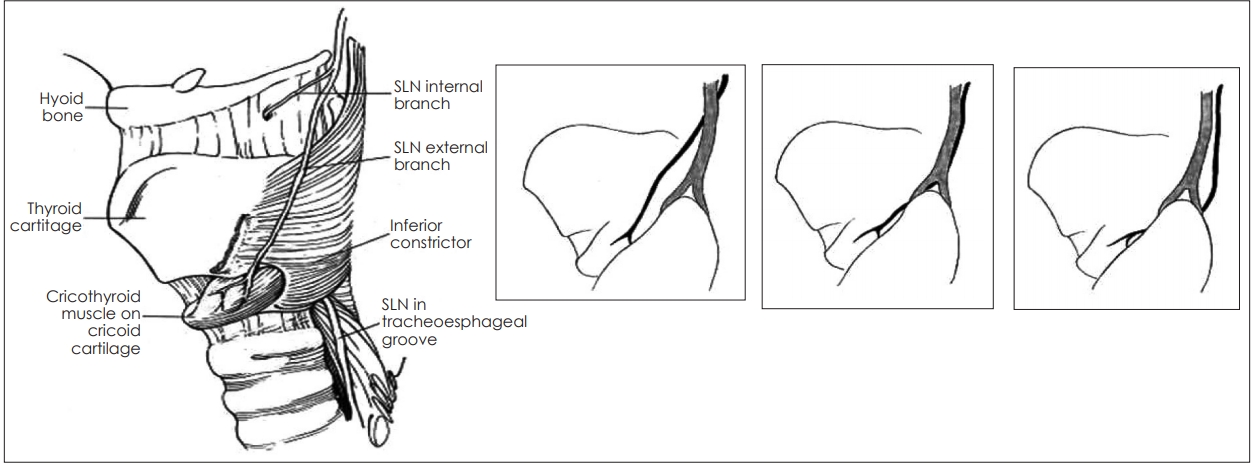
Table 1.
|
Neural |
Functional consequence |
Impact on voice character |
|
1. Recurrent laryngeal nerve (RLN) injury (complete or partial, transient or permanent) |
Immobile and laterally displaced fold |
Breathy voice, vocal fatigue, hoarseness |
|
Inadequate closure of vocal folds (VF) with phonation and swallowing |
|
Loss of VF bulk and tone |
|
Bowing of VF |
|
2. External branch of the superior laryngeal nerve (EBSLN) injury (complete or partial, transient or permanent) |
Physical findings are not good predictors but, if present, may include: |
Vocal fatigue, decreased ability to raise pitch, inability to project voice, decreased pitch flexibility and range |
|
• Posterior laryngeal rotation toward the paretic side, or shift of the petiole |
|
• Bowing of the VF on the weak side |
|
• Inferior displacement of the affected VF |
|
|
Non-Neural
|
Functional consequence
|
Impact on voice character
|
|
|
3. Direct cricothyroid muscle injurytransient myositis or direct injury |
As for EBSLN |
As for ESBLN |
|
4. Regional soft tissue injury (in the presence of intact neurological function) |
Laryngotracheal regional scar with fixation |
Voice fatigue, decrease in vocal range, speech becomes more monotone, vocal pitch can be lower |
|
Strap muscles denervation or trauma |
|
Local hematoma and/or edema |
|
5. Intubation-related injuries |
VF trauma (ie, edema, hematoma, laceration) |
Hoarseness, odynophagia |
|
General : 6-13% |
VF granuloma |
|
Vocal fold paresis (VFP) : .04% |
Arytenoid dislocation |
|
6. Voice change from unrelated intercurrent upper respiratory tract infection (URTI) |
Typically viral-related laryngitis unrelated to surgery, rarely associated with VFP |
Hoarseness, breathy voice if VFP |
Table 2.
갑상선 수술 후 발생한 일측성 성대마비의 치료 [ 2]
|
Procedure |
Effect |
Benefit |
Notes |
|
Voice Therapy by a speechlanguage pathologist |
Temporary or permanent improvement |
Adjustment and compensation to altered laryngeal physiology |
Exercises to improve the voice and/or swallowing |
|
Noninvasive treatment |
|
Injection laryngoplasty-injection of material into the vocal fold |
Temporary (typically months) |
Restores vocal fold position and bulk |
Can be repeated when the injection material disappears |
|
Often can be performed in the office, but may also be performed in the operating room |
|
Framework procedures-operations to improve vocal fold position |
Permanent |
Restores vocal fold position |
Near immediate restoration of Voice |
|
Some consider potentially reversible |
Performed in the operating room and requires a neck incision |
|
Reinnervation-an operation to improve vocal fold position |
Permanent |
Restores vocal fold position and bulk |
The final surgical outcome can take up to a year |
|
True restoration of physiologic reinnervation is not achievable |
A vocal fold injection is typically performed at the same time to rehabilitate voice during this healing period |
|
Performed in the operating room and requires a neck incision |
REFERENCES
1. Moris D, Mantonakis E, Makris M, Michalinos A, Vernadakis S. Hoarseness after thyroidectomy: blame the endocrine surgeon alone? Hormones (Athens) 2014; 13: 5- 15.    2. Chandrasekhar SS, Randolph GW, Seidman MD, et al. Clinical practice guideline: improving voice outcomes after thyroid surgery. Otolaryngol Head Neck Surg 2013; 148: 1- 37. 3. Chung EJ, Park MW, Cho JG, et al. A prospective 1-year comparative study of endoscopic thyroidectomy via a retroauricular approach versus conventional open thyroidectomy at a single institution. Ann Surg Oncol 2015; 22: 3014- 21. 4. Hong KH. Post-Thyroidectomy Syndrome. Korean J Otorhinolaryngol-Head Neck Surg 2014; 57: 297- 303.
|
|











