대동맥궁 동맥류에 의해 발생한 좌측 성대마비 1예 : Ortner 증후군
A Case of Left Vocal Cord Paralysis Caused by Aortic Arch Aneurysm : A Variant of Ortner's Syndrome
Article information
Abstract
Ortner's syndrome is a rare clinical entity with hoarseness attributable to recurrent laryngeal nerve palsy in cardiovascular diseases. The mechanism of this condition is thought to be due to compression of the recurrent laryngeal nerve by a dilated, tense cardiovascular structure against its adjacent tissue; thus, this is also known as cardio-vocal syndrome. We experienced the case of a 81-year-old female suffering from hoarseness due to a large aneurysm of the aortic arch, and reviews the literature for possible cardiovascular causes of Ortner's syndrome.
Introduction
Hoarseness due to vocal cord paralysis is related with injury to the recurrent laryngeal nerve (RLN). Two cases of left RLN paralysis in association with mitral stenosis were first described by Norbert Ortner, in 1897 [1]. Since then, an increasing number of cases showing a similar association between left RLN and cardiovascular diseases including mitral stenosis have been reported and called “Ortner’s syndrome” or “cardio-vocal syndrome” [2]. Among the previously reported cases, mitral stenosis was the most common underlying disease of Ortner’s syndrome. Other reports suggest left RLN paralysis can be caused by various clinical conditions including left ventricular failure, atrial septum failure, arterial canal persistency, primary pulmonary hypertension, pulmonary artery relapsing embolism, left ventricular aneurysm and various type of the aortic aneurysm [3-6]. It is rare that other cardiovascular diseases are responsible for the development of this syndrome [2]. Here, we report a case of hoarseness that was shown to be associated with left vocal cord paralysis due to the compression of the left RLN by an aortic arch aneurysm.
Case
A 81-year-old, non-smoking woman visited our clinic because of a 1-month history of hoarseness. He had neither a history of constitutional symptoms nor cardiorespiratory complaint. She had a long history of hypertension for 30 years. She denied any symptoms of aspiration, dysphagia, odynophagia or weight loss. Clinical examination revealed no obvious head and neck lymphadenopathy. Flexible laryngoscopy identified the cause of the hoarseness to be a paralyzed left vocal cord, in the para-median position (Fig. 1A).
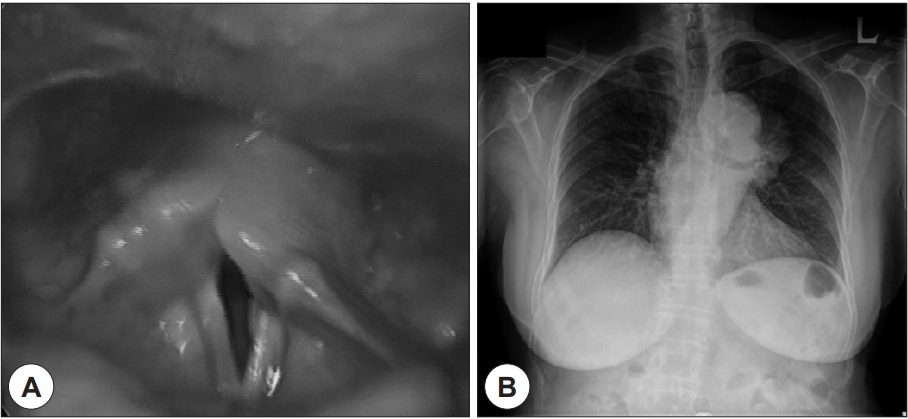
(A) Laryngoscopic finding presented left vocal fold paralysis with para-median position, and (B) chest radiography showed welldefined lobulated mediastinal lesion in left middle lung field abutting aortic arch with mild cardiomegaly.
Chest radiography showed widening of the mediastinum, and an anterior mediastinal mass or aortic aneurysm was suspected (Fig. 1B). The patient was admitted to the hospital for further examination. The results of cardiac auscultation and electrocardiography were normal. A contrast-enhanced computed tomography image of the chest revealed a saccular aneurysm of aortic arch that measured 7×6×5.1 cm, and extending posteriorly (Fig. 2). The lungs were otherwise unremarkable. It was thought that the left recurrent laryngeal nerve was compressed between the aortic aneurysm and the pulmonary artery or aortic ligament. A cardiothoracic surgical opinion was arranged. After consideration of the patient’s substantial risk of perioperative morbidity, she was discharged while receiving medical therapy for strict blood-pressure control. Instead of the surgical intervention for the aortic arch aneurysm, she received injection of hyaluronic acid into the left true vocal cord for improvement in voice quality.
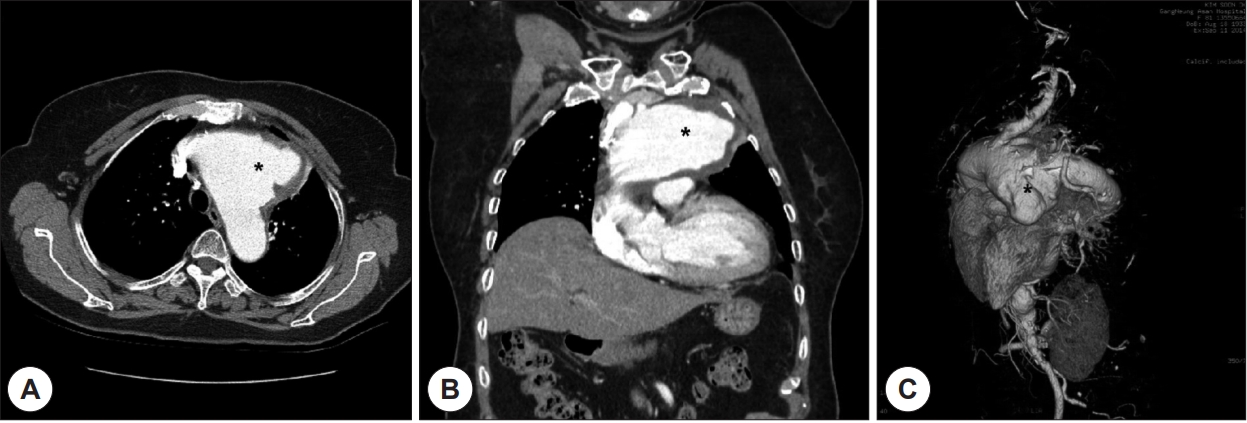
Contrast-enhanced axial computed tomography scan of the chest showing (A) axial view, (B) coronal view and (C) three-dimensional image. It reveals about 7×6×5.1 cm sized an enhancing saccular aneurysm arising from the arch of aorta with peripheral thrombus (* : the aneurysm).
Discussion
Ortner first described this syndrome in 1897 after seeing 2 patients with mitral stenosis and left atrial dilatation. Although Ortner’s syndrome initially was described for cardio-vocal hoarseness due to an enlarged left atrium, but over the years it has been used by many authors to describe cardio-vocal hoarseness caused by cardiovascular causes [1,2]. Specifically, RLN injury is secondary to compression caused by changes in the anatomy of the heart or great vessels [7].
Understanding the pathophysiology of cardio-vocal syndrome mandates a review of the anatomy of RLN. On the right side, it crosses the first part of the subclavian artery and hooks around to travel between the trachea and esophagus. On the left side, the RLN arises from the left vagus nerve at the anterolateral border of the aortic arch in a space between the main pulmonary artery and aortic arch, just behind the ligamentum arteriosum, and ascends in the groove between the trachea and esophagus [8]. Therefore, a dilated pulmonary artery or a persistent ductus arteriosus or an aneurysm of the aortic arch may lead to compression of the nerve. The exact mechanism of RLN paralysis in cardio-vocal syndrome has been a subject of debate [2,9]. Ortner initially postulated that an enlarged left atrium pushing upwards on the left RLN and compressing the nerve against the arch of aorta was responsible for the paralysis [1]. However, a series of subsequent anatomical and radiological studies disputed this hypothesis and indicated that the nerve is compressed between the pulmonary artery and a dilated lesion of the aorta arch [10]. On the basis of Cadaveric studies, Fetterrolf and Norris presented that in Ortner’s syndrome the nerve is compressed between the aorta, ligamentum arteriosum and the left pulmonary artery, as the distance between the aorta and the pulmonary artery in the aorto-pulmonary window is only 4 mm [11].
The incidence of aortic aneurysms has been reported to be 12.5 per 100,000 person/year [12]. In patients with hoarseness, 11% of the cases have idiopathic or rare causes of hoarseness which include cardio-vocal hoarseness [2]. In this point of view, aortic arch aneurysm presenting as hoarseness is extremely rare case of our patient. The aneurysms of the aorta can be traumatic, saccular, atherosclerotic, mycotic, and pseudoaneurysm and can have an associated dissection [13]. Patients with expanding or symptomatic aneurysms larger than 6cm should undergo surgery. Our patient’s saccular aneurysm of the aortic arch was relatively large (7×6×5.1 cm) but asymptomatic. She had only history of hypertension. However, she underwent no any surgical treatment because of the patient’s substantial risk of perioperative morbidity.
Information regarding the reversibility of hoarseness in cardio-vocal syndrome after correction of the underlying cardiovascular disease is limited. Of those previously reported, 85.7% cases resolved within 1 week to 3 years, with duration of preexisting hoarseness ranging from 1 month to 10 years. The chance of recovery, however, might depend on the degree and duration of RLN [2,8,14]. Our patient suffered from hoarseness for 1 month, and her voice was improved after injection laryngoplasty, instead of surgical intervention.
Hoarseness is commonly encountered in the otolaryngology outpatient clinic ; however, cardio-vocal hoarseness is an unusual presentation [3]. The otolaryngologist should consider the diagnosis of Ortner’s syndrome after more common causes have been excluded, particularly in the elderly or patients with cardiovascular disease. This case presentation is intended to present that the suspicion of cardio-vocal syndrome should be highly kept in mind in patient with hoarseness of voice in the elderly.