기관절개술과 후두절개술로 치료한 거대 성문하 용종 1예
Huge Subglottic Polyp Treated with Tracheotomy and Laryngofissure
Article information
Trans Abstract
Vocal polyps are benign laryngeal lesions which arise from the Reinke’s space abd hoarseness is the most common symptom. However, airway compromised is rarely presented in the vocal polyp. A rare case of large subglottic polyp causing dyspnea is reported. Tracheostomy was performed under local anesthesia and then the mass was resected under general anesthesia using a laryngofissure approach. The dyspnea and hoarseness disappeared after surgery immediately. The histopathological findings indicated a diagnosis of vocal cord polyp with chronic inflammatiuon. We consider that tracheostomy is the safest and most useful procedure to guarantee the upper airway in cases of large vocal polyp showing dyspnea. We hereby report a case of huge subglottic polyp in which a tracheostomy and laryngofissure was required for removing the subglottic mass successfully.
Introduction
Vocal cords polyp is one of the most common benign mucosal lesions that arise from the true vocal cords. The main etiologies are due to voice abuse/disuse, smoking, allergy, gastroesophageal reflux and chronic infection. It occurs frequently when the patients require occupationally an excessive usage of voice. Most of the cases are reported to be unilateral polyp, but can be bilateral or multiple unilateral. The symptoms could be variable such as dysphonia, foreign body sensation, wheezing, stridor and even upper airway obstruction. It depends on the size and site of the polyps [1,2].
Very rarely, there could be airway compromise and emergency airway managements reported due to large vocal cord polyp. When the polyps appear at the subglottic area, the hanging polyp would flop and follow the rhythm of respiration. And there is a possibility of airway obstruction and laryngospasm due to huge vocal polyp when there are any bouts of coughing, vomiting or any manipulation at the laryngeal inlet [3-5]. We should be aware of the possibility of upper airway obstruction when a patient has a dyspnea and voice. Generally, tracheostomy is performed and microlaryngoscopic excision of the polyp is the preferred treatment. Meticulous treatment by otolaryngologist and anaesthetist should be mutually carried out in cases of huge vocal polyp causing airway obstruction
Case Report
A 48-year-old man visited emergency room with severe dysphonia and dyspnea for 3 days with increased severity. His past history was not significant, with no history of surgery, bur heavy smoker for more than 30 years. No lesion was evident in the oral cavity, oropharynx, and other head and neck regions. He could not lie down and had noisy breathing during inspiration. Mild cyanosis was detected on the face and lips. He had sometimes coughing and hemoptysis, but odynophagia and dysphagia were not noted. He was a chronic smoker for more than 20 years (1 pack/day). Other systemic disease was not noted and general condition was well till this hospitalization. On physical examination, he showed a mildly tachypnea. A biphasic inspiratory stridor was noted with suprasternal recession. No neck mass were detected. A fiberoptic laryngeal examination revealed a reddish mass occupying glottis area. A mass was flopping with respiration, almost blocking the whole glottis area. Other supraglottic area, epiglottis, vallecular, base of tongue and pyriform sinus, were normal. Computed tomography showed 2 cm sized subglottic mass with irregular shape, but not glottis level. A mass was not enhanced with contrast CT images (Fig. 1). The cervical lymph nodes were not noted. This mass almost obstructed the airway. A difficult intubation was anticipated and a tracheostomy under local anesthesia was performed. After tracheotomy we tried to remove the mass under laryngeal microsurgery, but failed to remove the mass. Then we decided to open the larynx with laryngofissure. A mass originated on the under surface of left vocal fold and removed without difficulty. The histopathological finding revealed vocal polyp[ with chronic inflammatory. Postoperatively laryngoscopy revealed no residual and airway was adequate. The vocal folds were well mobile and airway was good patent, therefore decannulation of tracheostomy was done. The mild left subglottic edema and redness was noted at 7 days after surgery (Fig. 2). The patient was followed up for one month. On examination of the larynx, there was small polyp at the anterior 1/3 of the right vocal cord with an adequate airway.
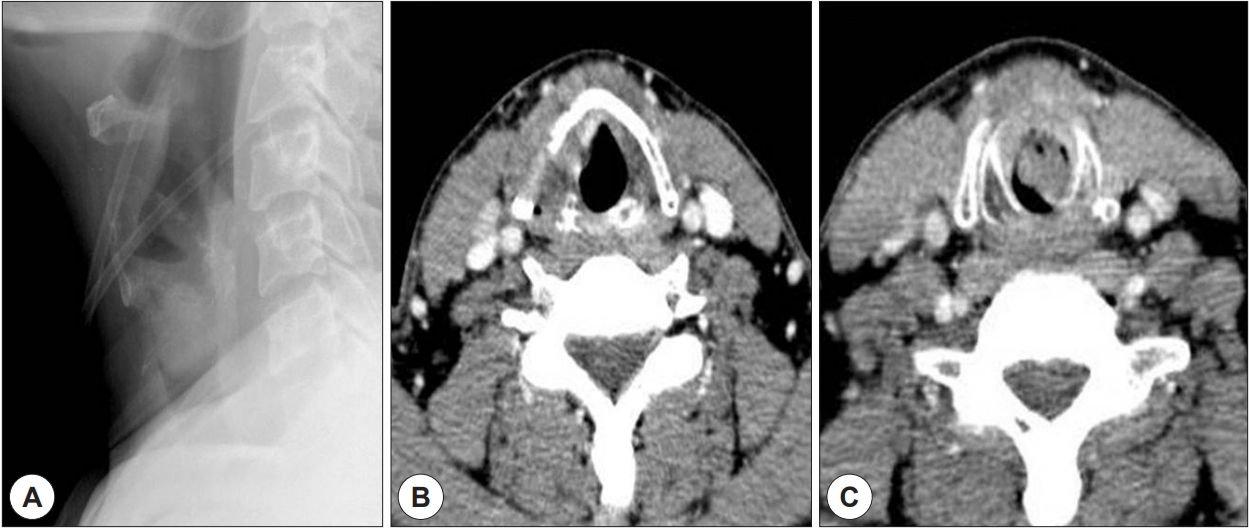
Neck lateral X-ray shows the large mass at the subglottic space (A). Axial CT scan at the level of the glottis (B) and subglottis (C) shows the large mass that nearly obstructed the airway lumen on the subglottic area.
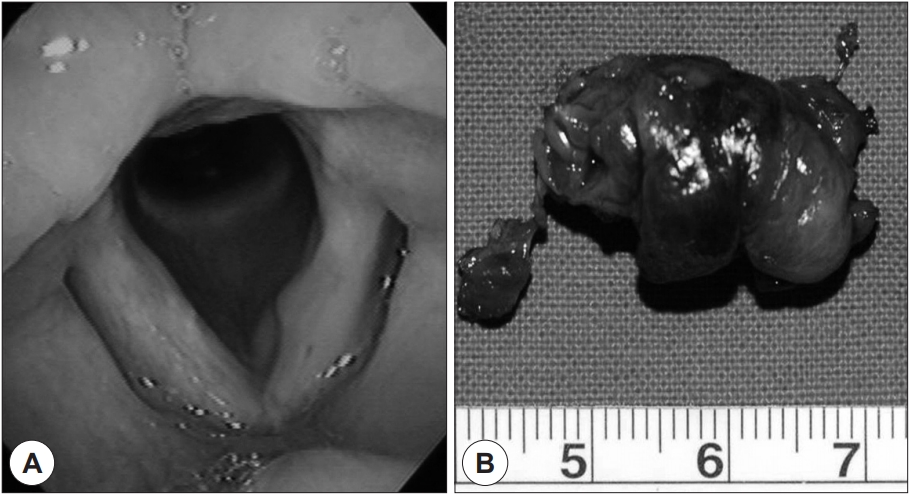
Laryngoscopic finding, left subglottic swelling after surgery (A), and excised surgical specimen (B).
Discussion
Vocal polyp occurs along the membranous vocal folds and usually located at the mid portion of the membranous vocal fold. Generally ,vocal polyp usually presents as an exophytic or pedunculated lesion with thin mucosa. Reinke’s edema, polyps and nodules are into the same entity based on their similar histological findings. As for Reinke’s edema, it occurs by accumulation of fluid of variable viscosity, commonly effects bilateral vocal cords and vibration could be observed during phonation [1,2]. Generally, a small polyp or hemorrhagic polyp is not indicated for any surgical intervention. But surgical intervention is mandatory in cases which not improve after long term voice rest or cause airway obstruction. In the treatment of vocal polyps, microlaryngeal surgery under general anesthesia is the definitive management.
The primary symptom in patients with a vocal cord polyp is usually voice change, but large vocal cord polyps can present additionally with respiratory symptoms such as respiratory distress. Benign vocal inflammatory polyps are very common, but respiratory distress is rare. But, life threat by airway obstruction is extremely unusual due to the large laryngeal polyp. A rare case of death due to a large laryngeal polyp has been reported in the literature. The remaining small glottis area results in difficult intubation or complicated intubation. In this situation, there was limitation to expose a glottis and hence multiples attempts of intubation might be warranted. These cause further injuries to the membranous vocal folds or cartilage injury such as arytenoid dislocation. The risk of laryngospasm during the intubation carries certain morbidity and mortality. In addition, it is possible to dislodge the polyp during endotracheal intubation due to the narrow space [6,7]. Therefore, tracheostomy under local anesthesia might to be a better choice in this case.
On considering the size and location of the large polyp, tracheostomy was preferred for safe intubation of general anesthesia. An endotracheal intubation lead to dislodgement of the polyp and cause acute airway obstruction. After tracheostomy for general anesthesia, the vocal polyp could be excised by laryngeal microsurgery [6,7]. In this case, we primarily expected the cause of acute airway obstruction is due to laryngeal mass such as tumor because a patients had smoked for more than 20 years. We decided to open of the larynx with laryngofissure approach. In conclusion, hoarseness may be the only complaint from the patient when the lesion is small, but big vocal polyps will lead to severe airway obstruction and even fatality.