ņä£ ļĪĀ
ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØĆ ļō£ļ¼╝Ļ▓ī ļéśĒāĆļéśļŖö ļ╣äĻ░ĢņØś ņ¢æņä▒ ņóģņ¢æņ£╝ļĪ£ ņĀäņ▓┤ ļ╣äĻ░Ģ ņóģņ¢æņØś 0.5~4%ļź╝ ņ░©ņ¦ĆĒĢ£ļŗż. ņŻ╝ļĪ£ ļ╣äĻ░ĢņØś ņĖĪļ▓ĮņØ┤ļéś ļČĆļ╣äļÅÖņŚÉņä£ ņ”ØņŗØļÉ£ ņāüĒö╝ņäĖĒżĻ░Ć ļ░śņĀäņä▒ņ£╝ļĪ£ ĻĖ░ņ¦ł ļé┤ļĪ£ ņä▒ņןĒĢśņŚ¼ ļ░£ņāØĒĢ£ļŗż[1]. ņØ┤ļ¤¼ĒĢ£ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØĆ ņŻ╝ļĪ£ 40~70ņäĖņŚÉ ļ░£ņāØĒĢśļ®░ ņåīņĢäļéś ņ▓ŁņåīļģäĻĖ░ņŚÉļŖö ļō£ļ¼Ė Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ£╝ļ®░, ļé©ļģĆ ļ╣äļŖö 4:1ļĪ£ ļ│┤Ļ│ĀļÉ£ļŗż[2]. ļ│æļ”¼ĒĢÖņĀüņ£╝ļĪ£ ņ¢æņä▒ ņóģņ¢æņØ┤ņ¦Ćļ¦ī ņ×¼ļ░£ļźĀņØ┤ ļåÆĻ│Ā Ļ│© ļ░Å ņŻ╝ņ£ä ņĪ░ņ¦üņØä ĒīīĻ┤┤ĒĢĀ ņłś ņ׳ņ£╝ļ®░, ņĢģņä▒ ņóģņ¢æĻ│╝ņØś ņŚ░Ļ┤Ćņä▒ņØ┤ ņĄ£ļīĆ 15%Ļ╣īņ¦Ć ņ׳ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ¢┤ ņ×äņāüņĀüņ£╝ļĪ£ļŖö ņĢģņä▒ ņóģņ¢æĻ│╝ Ļ░ÖņØ┤ ņĘ©ĻĖēļÉśĻ│Ā ņ׳ņ£╝ļ®░ Ļ┤æļ▓öņ£äĒĢ£ ņłśņłĀņĀü ņĀ£Ļ▒░ ļ░Å ņ¦ĆņåŹņĀüņØĖ ņČöņĀüņØ┤ ĒĢäņÜöĒĢśļŗż[3].
ļ╣äĻ░Ģ ņØ┤ņÖĖņŚÉņä£ņØś ļ░£ņāØņØĆ ļō£ļ¼Ė Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ£╝ļéś ņØ╝ļČĆ ļ¼ĖĒŚīņŚÉņä£ ļ╣äĻ░Ģ ņÖĖ ļ░£ņāØņØ┤ ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ļŗż. SwaidņÖĆ Alsaied [4]ļŖö ņä▒ļ¼ĖņāüņŚÉņä£ ļ░£ņāØĒĢ£ ļ░śņĀäņä▒ ņ£ĀļæÉņóģ 1ņśłļź╝ ņĄ£ņ┤łļĪ£ ļ│┤Ļ│ĀĒĢ£ ļ░ö ņ׳ņ£╝ļéś, ņØ┤Ēøä ļ│┤Ļ│ĀļÉ£ ļ░ö ņŚåļŗż. ņØ┤ņŚÉ ļ│Ė ņ”ØļĪĆļ│┤Ļ│ĀņŚÉņä£ļŖö ĻĄŁļé┤ņŚÉņä£ ņĄ£ņ┤łļĪ£ ĒÖĢņØĖļÉ£ ņä▒ļ¼ĖņāüņØś ļ░śņĀäņä▒ ņ£ĀļæÉņóģ 1ņśłļź╝ ļ│┤Ļ│ĀĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ņ”Ø ļĪĆ
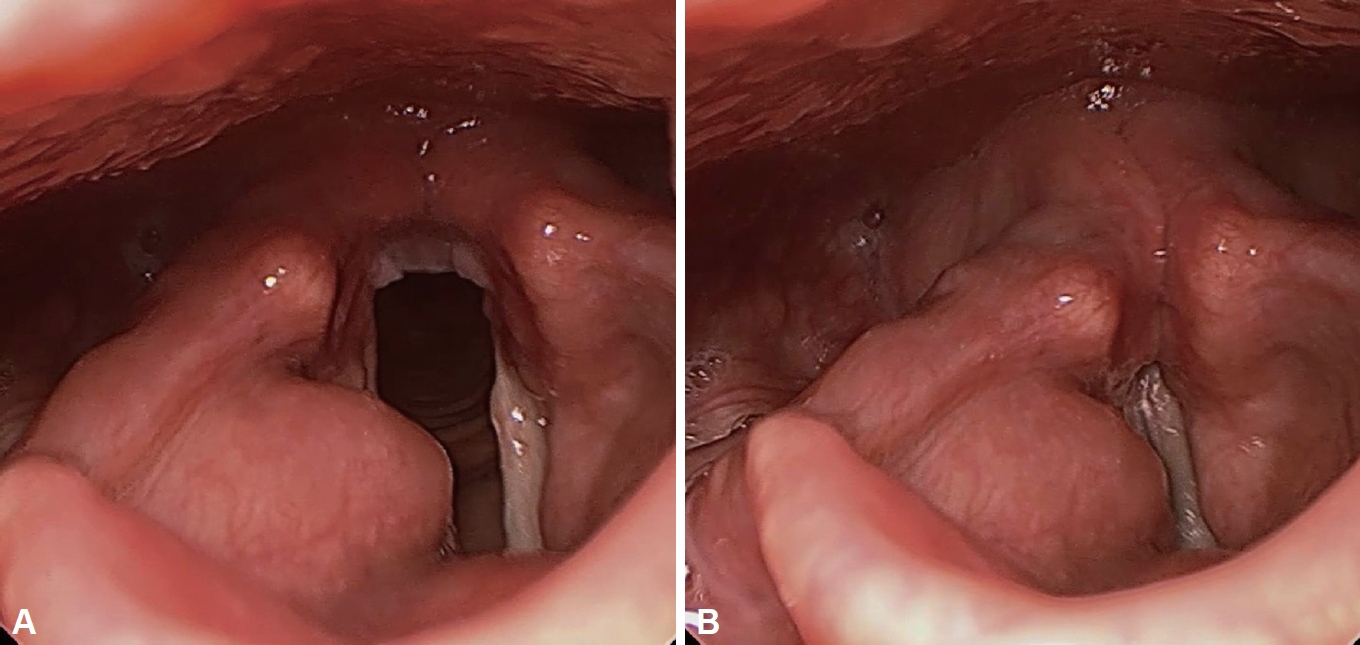
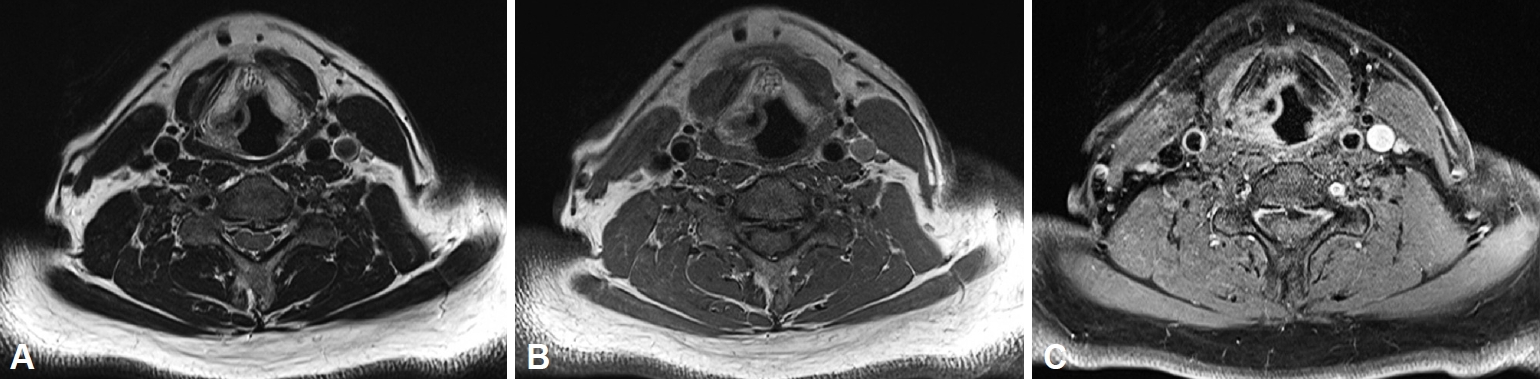
62ņäĖ ļé©ņ×É ĒÖśņ×ÉĻ░Ć ļé┤ņøÉ 2Ļ░£ņøö ņĀäļČĆĒä░ ļ░£ņāØĒĢ£ Ļ▓ĮļČĆ ņØ┤ļ¼╝Ļ░ÉņØä ņŻ╝ņåīļĪ£ ļ│ĖņøÉ ņÖĖļלņŚÉ ļé┤ņøÉĒĢśņśĆļŗż. ņÖĖļלņŚÉņä£ ņŗ£Ē¢ēĒĢ£ ĒøäļæÉļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ņāü ņÜ░ņĖĪ Ļ░Ćņä▒ļīĆņŚÉ ņ¦üĻ▓Į 2 cmĻ░Ćļ¤ēņØś ņóģļ¼╝ņØ┤ ĒÖĢņØĖļÉśņŚłļŗż(Fig. 1). Ļ▓ĮļČĆ ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśüņāü Ļ▓ĮĻ│ä ļČĆņ£äņŚÉ ņĪ░ņśüņØ┤ ņ”ØĻ░ĢļÉśĻ│Ā ļé┤ļČĆņŚÉ Ļ▓®ļ▓ĮņØ┤ ļÅÖļ░śļÉ£ ņåīņŚĮņāüņØś(lobulated) ļéŁņä▒ ļ│æļ│ĆņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 2). ņØ┤Ēøä, Ļ▓ĮļČĆ ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāüņØä ņ┤¼ņśüĒĢśņśĆĻ│Ā T2 Ļ░ĢņĪ░ņśüņāüņŚÉņä£ ņżæļō▒ļÅäņØś ņŗĀĒśĖļź╝ ļ│┤ņśĆļŗż(Fig. 3). ņ×äņāü ļ░Å ņśüņāüĻ▓Ćņé¼ņāü ĒøäļæÉļéŁņóģ(laryngocele) Ļ░ĆļŖźņä▒ņØ┤ ļåÆļŗżĻ│Ā ĒÖĢņØĖļÉśņ¢┤, ņĪ░ņ¦üĻ▓Ćņé¼ ļ░Å ņ╣śļŻī ļ¬®ņĀüņ£╝ļĪ£ ĒøäļæÉļ»ĖņäĖĒśäļ»ĖĻ▓ĮĒĢś ļĀłņØ┤ņĀĆ ņĀłņĀ£ņłĀņØä ņĀäņŗĀļ¦łņĘ©ĒĢśņŚÉ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņ¢æņä▒ ņóģņ¢æņØś ņłśņłĀņŚÉ ņżĆĒĢśņŚ¼ ņóģņ¢æņØś Ļ▓ĮĻ│äļź╝ ļö░ļØ╝ ņĀłņĀ£ĒĢśņśĆņ£╝ļ®░, ņłśņłĀ ņżæ ļÅÖĻ▓░ņĀłĒÄĖĻ▓Ćņé¼ļŖö ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņĢśļŗż. ņóģļ¼╝ ņĀłņĀ£ ņØ┤Ēøä, ņĀłņĀ£ņŚ░ņØ┤ ņØ╝ļČĆļČä ļŗ©ļŗ©ĒĢśĻ▓ī ļ¦īņĀĖņ¦ĆļŖö Ļ▓āņØä ĒÖĢņØĖĒĢśņśĆņ£╝ļ®░, ņłśņłĀ Ēøä ņĄ£ņóģ ļ│æļ”¼Ļ▓Ćņé¼ Ļ▓░Ļ│╝ņŚÉ ļö░ļØ╝ ĒĢäņÜö ņŗ£ ņČöĻ░ĆņĀüņØĖ ņ╣śļŻī Ļ│äĒÜŹņØä ņłśļ”ĮĒĢśĻĖ░ļĪ£ ĒĢśņśĆļŗż.
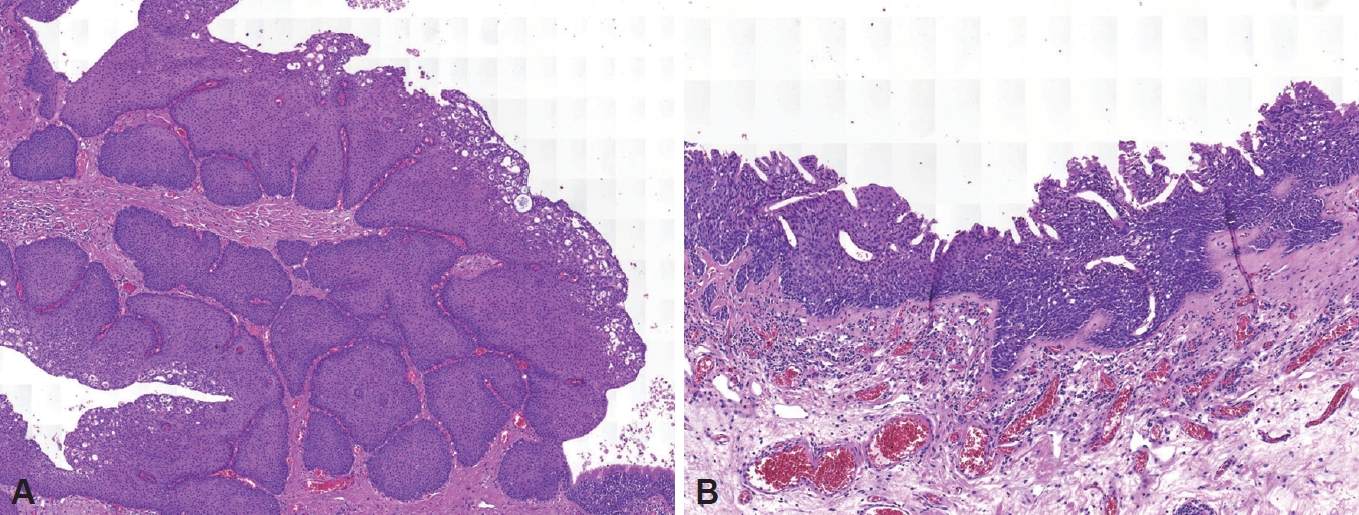
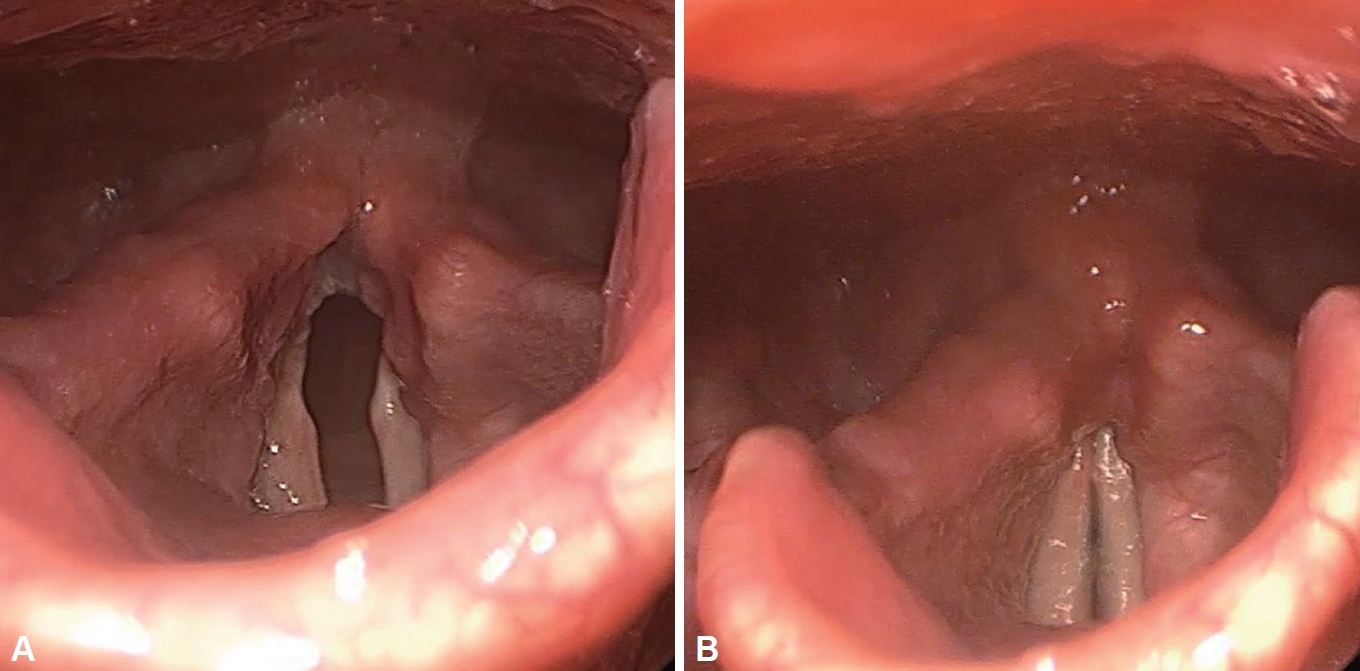
ņłśņłĀ Ēøä hematoxylin and eosin ņŚ╝ņāēņØä ĒåĄĒĢ£ ļ│æļ”¼Ļ▓Ćņé¼ Ļ▓░Ļ│╝, Ļ│╝ĒśĢņä▒ļÉ£ ĒÄĖĒÅēņāüĒö╝ņäĖĒżĻ░Ć ĻĖ░ņ¦ł ļé┤ļĪ£ ļé┤ļ▓łĒĢśļŖö ņ¢æņāüņØ┤ ĒÖĢņØĖļÉśņ¢┤ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņ£╝ļĪ£ ņ¦äļŗ©ļÉśņŚłļŗż(Fig. 4). Ēśäņ×¼ ņłśņłĀ Ēøä ņĢĮ 3Ļ░£ņøö Ļ▓ĮĻ│╝ĒĢ£ ņāüĒā£ļĪ£ Ļ▓ĮļČĆ ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśü ļ░Å ĒøäļæÉļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ņāü ņ×¼ļ░£ ļ░Å ĒĢ®ļ│æņ”Ø ņŚåņØ┤ ņל ņ╣śņ£ĀļÉ£ ņåīĻ▓¼ņØä ļ│┤ņśĆļŗż(Fig. 5).
Ļ│Ā ņ░░
ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØĆ ņÖĖļ░░ņŚĮ ĻĖ░ņøÉņØś ņä¼ļ¬©ĒśĖĒØĪņāüĒö╝ņØĖ schneiderian ņāüĒö╝ņŚÉņä£ ļ░£ņāØĒĢśļ®░ ņŻ╝ļĪ£ ļ╣äļČĆļ╣äĻ░Ģ ļé┤ņŚÉ ļ░£ņāØĒĢ£ļŗż[5]. Schneiderian ņāüĒö╝ņŚÉņä£ ļ░£ņāØĒĢ£ ņ£ĀļæÉņóģņØĆ ĻĘĖ ņä▒ņן ņ¢æņŗØņŚÉ ļö░ļØ╝ ļ░śņĀäņä▒(inverted), ļ▓äņä» ļ¬©ņ¢æ(fungiform), ņøÉĒåĄĒśĢ(cylindrical) ņ£ĀļæÉņóģņ£╝ļĪ£ ļéśļē£ļŗż[5].
ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ļ│æņØĖņØĆ ļ¬ģĒÖĢĒĢśĻ▓ī ņĢīļĀżņĀĖ ņ׳ņ¦Ć ņĢŖņ£╝ļéś, ļ░śņĀäņä▒ ņ£ĀļæÉņóģ Ļ▓Ćņ▓┤ņŚÉņä£ ņØĖņ£ĀļæÉņóģļ░öņØ┤ļ¤¼ņŖż(human papilloma virus, HPV), ĒīīĒżļ░öļ░öņØ┤ļ¤¼ņŖż(papovavirus)ņÖĆ Ļ░ÖņØĆ ļ░öņØ┤ļ¤¼ņŖż Ļ▓ĆņČ£ņØ┤ ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ļŗż[6]. ĒŖ╣Ē׳, ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ĒśĢņä▒, ņ×¼ļ░£, ņĢģņä▒ ļ│ĆĒÖöņÖĆ ņØĖņ£ĀļæÉņóģļ░öņØ┤ļ¤¼ņŖżņØś ņŚ░Ļ┤Ćņä▒ņØ┤ ņĢīļĀżņĀĖ ņ׳ļŗż[7]. Caruana ļō▒[8]ņØĆ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś 38%, ņØ┤ĒśĢņä▒ņØä ļ│┤ņØ┤ļŖö ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś 50%ņŚÉņä£ ņØĖņ£ĀļæÉņóģļ░öņØ┤ļ¤¼ņŖżĻ░Ć Ļ▓ĆņČ£ļÉśņŚłļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż. HPV typeņØĆ ņóģņ¢æņøÉņä▒(oncogenicity)ņØä ĻĖ░ņżĆņ£╝ļĪ£ ņĀĆņ£äĒŚśļÅäņÖĆ Ļ│Āņ£äĒŚśļÅäļĪ£ ĻĄ¼ļČäĒĢśļŖöļŹ░, ņĀĆņ£äĒŚśļÅäņØś HPV 6Ļ│╝ HPV 11 ņ┤łĒÜīĻ░ÉņŚ╝ņØ┤ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ļ░£ņāØĻ│╝ ņŚ░Ļ┤ĆņØ┤ ņ׳Ļ│Ā ņØ┤Ēøä Ļ│Āņ£äĒŚśļÅäņØś HPV 16Ļ│╝ HPV 18 Ļ░ÉņŚ╝ņØ┤ ņĢģņä▒ ļ│ĆĒÖö(ĒÄĖĒÅēņØ┤ĒśĢņä▒ ļśÉļŖö ĒÄĖĒÅēņäĖĒżņĢö)ļź╝ ņØ╝ņ£╝Ēé¼ ņłś ņ׳ļŗż[7].
Ēśäņ×¼Ļ╣īņ¦Ć ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤, ņżæņØ┤, ņ£Āņ¢æļÅÖ, ņĖĪļæÉĻ│©, ļłłļ¼╝ņŻ╝ļ©Ėļŗł, ļ╣äņØĖļæÉ, ĻĄ¼ņØĖļæÉ, ĒĢśņØĖļæÉ, ĻĄ¼Ļ░Ģ, ĻĖ░Ļ┤Ć, ĒÅÉ ļō▒ņŚÉ ņØ┤ņåīņä▒ ļ░śņĀäņä▒ ņ£ĀļæÉņóģ ļ░£ņāØņØ┤ ļ│┤Ļ│ĀļÉśņŚłļŗż. ļ╣äĻ░Ģ ņØ┤ņÖĖņŚÉņä£ ļ░£ņāØĒĢ£ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ļ│æņØĖņØĆ ļ¬ģĒÖĢĒ׳ ņĢīļĀżņĀĖ ņ׳ņ¦Ć ņĢŖļŗż. ļ╣äļČĆļ╣äĻ░Ģ ļé┤ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ņ¦üņĀæ ņ╣©ļ▓ö(direct extension)ņŚÉ ņØśĒĢ┤ ņżæņØ┤, ļ╣äņØĖļæÉ, ĻĄ¼ņØĖļæÉņØś ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØ┤ ļ░£ņāØĒĢĀ ņłś ņ׳ļŗż[9]. ņ¦üņĀæ ņ╣©ļ▓öņØś ņ”ØĻ▒░Ļ░Ć ņŚåļŖö ļ╣äĻ░Ģ ņØ┤ņÖĖņØś ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ļ│æņØĖņ£╝ļĪ£ļŖö ņØ┤ņåīņä▒ Ēæ£Ēśä(ectopic expression)ņØä Ļ│ĀļĀżĒĢĀ ņłś ņ׳ļŗż[9]. ļśÉĒĢ£, ļ╣äļČĆļ╣äĻ░Ģ ļé┤ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ņłśņłĀ Ļ│╝ņĀĢņŚÉņä£, ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØ┤ ņĀäĒīīļÉĀ ņłśļÅä ņ׳ļŗż[10]. ļ│Ė ņ”ØļĪĆņŚÉņä£ļŖö ļ╣äļČĆļ╣äĻ░Ģ ļé┤ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ņ×äņāüņĀü ņ”ØĻ▒░ļŖö ņŚåņŚłņ£╝ļ®░, ĒøäļæÉņØś ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ļ¬ģĒÖĢĒĢ£ ļ│æņØĖņØä ĒīīņĢģĒĢĀ ņłśļŖö ņŚåņŚłļŗż.
ĒøäļæÉņØś ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ļ░£ņāØņØĆ ĻĘ╣Ē׳ ļō£ļ¼Ė Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. Saddawi-Konefka ļō▒[11]ņŚÉ ļö░ļź┤ļ®┤, ņØīņä▒ ļ│ĆĒÖöļź╝ ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢ£ 59ņäĖ ņŚ¼ņä▒ ĒÖśņ×ÉņŚÉņä£ 1.5 cm Ēü¼ĻĖ░ņØś ņóīņĖĪ Ļ░Ćņä▒ļīĆ ņóģļ¼╝ņØ┤ ĒÖĢņØĖļÉśņ¢┤ ņŗ£Ē¢ēĒĢ£ ņĪ░ņ¦üĻ▓Ćņé¼ņāü ņä▒ļ¼Ėņāü ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØ┤ ņĄ£ņ┤łļĪ£ ĒÖĢņØĖļÉ£ ļ░ö ņ׳ļŗż. ļśÉĒĢ£, SwaidņÖĆ Alsaied [4]ļŖö ņ▓£ļ¬ģņØīņØä ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢ£ 4ņäĖ ļé©ņ×É ĒÖśņ×ÉņŚÉņä£ ĻĖ░Ļ┤Ćņ¦Ćļé┤ņŗ£Ļ▓Įņāü ļé┤Ļ▓ĮņØś ņĢĮ 50%ļź╝ ņ░©ņ¦ĆĒĢśļŖö ņä▒ļ¼ĖĒĢśļČĆ ņóģņ¢æņØ┤ ĒÖĢņØĖļÉśņ¢┤ ņĀłņĀ£ Ēøä ņŗ£Ē¢ēĒĢ£ ņĪ░ņ¦üĻ▓Ćņé¼ņāü ņä▒ļ¼ĖĒĢś ļ░śņĀäņä▒ ņ£ĀļæÉņóģ 1ņśłļź╝ ņĄ£ņ┤łļĪ£ ļ│┤Ļ│ĀĒĢśņśĆļŗż. ļ╣äĻ░Ģ ņØ┤ņÖĖņŚÉ ļ░£ņāØĒĢśļŖö ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØ┤ ļ╣äĻ░Ģ ļé┤ ļ░śņĀäņä▒ ņ£ĀļæÉņóģĻ│╝ļŖö ĻĄ¼ļ│äļÉśļŖö ņ¦łļ│æņØĖņ¦ĆļŖö ļČłļČäļ¬ģĒĢśļŗż. Ēśäņ×¼Ļ╣īņ¦Ć ļ╣äĻ░Ģ ņØ┤ņÖĖņŚÉņä£ ļ░£ņāØĒĢ£ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņŚÉ ļīĆĒĢ£ ņ╣śļŻīļ▓ĢņØĆ ņĀĢļ”ĮļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖļŗż[11].
ņśüņāüņØśĒĢÖņĀüņ£╝ļĪ£, ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØĆ ņŻ╝ļĪ£ ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśüņØä ĒåĄĒĢ┤ ņ¦äļŗ©ļÉśņ¦Ćļ¦ī, ņóģņóģ ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśü ņśüņāüņŚÉņä£ ļ╣äņÜ®ņóģĻ│╝ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØä Ļ░Éļ│äĒĢśĻĖ░ ņ¢┤ļĀżņÜĖ ņłś ņ׳ļŗż. ņØ┤ļ¤¼ĒĢ£ Ļ▓ĮņÜ░, T2 Ļ░ĢņĪ░ ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāüņØä ĒåĄĒĢ┤ ļŹöņÜ▒ ņĀĢĒÖĢĒ׳ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØä Ļ░Éļ│äĒĢĀ ņłś ņ׳ļŗż[12]. ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØĆ ņןĻĖ░Ļ░äņØś ņ×äņāü Ļ▓ĮĻ│╝ļź╝ ļ│┤ņØ┤ļ®░, ļ╣äņÜ®ņóģņ£╝ļĪ£ ņśżņØĖļÉĀ Ļ▓ĮņÜ░ ņĀ£Ļ▒░ Ēøä ņĪ░ņ¦üĒĢÖņĀü Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦ÄĻĖ░ ļĢīļ¼ĖņŚÉ, ņ¦äļŗ©ļÉśņ¦Ć ņĢŖļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż[13].
ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ņĢģņä▒ĒÖöņ£©ņØĆ 5~15%ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[14]. ļ╣äļČĆļ╣äĻ░Ģ ļé┤ņØś ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś ņ╣śļŻīļ▓Ģņ£╝ļĪ£ Ļ│╝Ļ▒░ņŚÉļŖö ņĖĪļ╣äņĀłĻ░£ņłĀņØä ĒåĄĒĢ£ ņāüņĢģļÅÖņĀłņĀ£ņłĀ(lateral rhinotomy and maxillectomy), ņĢłļ®┤ņżæņĢÖņĀæĻĘ╝ļ▓Ģ(midfacial degloving approach), ļæÉĻ░£ņĢłļ®┤ņĀæĻĘ╝ļ▓Ģ(craniofacial approach)Ļ│╝ Ļ░ÖņØĆ Ļ┤æļ▓öņ£äĒĢ£ ĻĘ╝ņ╣śņĀü ņłśņłĀņØ┤ ņäĀĒśĖļÉśņŚłļŗż[15]. ņØ┤ļ¤¼ĒĢ£ Ļ┤æļ▓öņ£äĒĢ£ ĻĘ╝ņ╣śņĀü ņłśņłĀņØĆ ļ¦ÄņØĆ ĻĖ░ļŖźņĀü, ļ»ĖņÜ®ņĀü ĒĢ®ļ│æņ”ØņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ, ņĄ£ĻĘ╝ņŚÉļŖö ļé┤ņŗ£Ļ▓ĮņĀü ņ╣śļŻīĻ░Ć ņŻ╝ļĪ£ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŗż. Karkos ļō▒[13]ņØĆ ĻĘ╝ņ╣śņĀü ņ╣śļŻīņÖĆ ļé┤ņŗ£Ļ▓ĮņĀü ņ╣śļŻīļź╝ ļ╣äĻĄÉĒĢśņśĆĻ│Ā ļæÉ ĻĄ░ Ļ░äņŚÉ ņ×¼ļ░£ļźĀņŚÉ ņ£ĀņØśļ»ĖĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåņØīņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż.
ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØĆ ņ×¼ļ░£ļźĀņØ┤ ļåÆņØĆ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. ņóģņ¢æņØś ļŗżņżæņŗ¼ņä▒(multicentricity) ļ░Å ļČłņÖäņĀäĒĢ£ ņĀłņĀ£Ļ░Ć ļåÆņØĆ ņ×¼ļ░£ļźĀņØś ņŻ╝ņÜö ņøÉņØĖņØ┤ļŗż. ļīĆļČĆļČäņØś Ļ▓ĮņÜ░ ņłśņłĀ Ēøä 5ļģä ņØ┤ļé┤ ņ×¼ļ░£ĒĢśņ¦Ćļ¦ī, 10ļģä ņØ┤ĒøäņŚÉļÅä ņ×¼ļ░£ĒĢĀ ņłś ņ׳ņ¢┤ņä£ ņ¦ĆņåŹņĀüņØĖ Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ņØ┤ ĒĢäņÜöĒĢśļŗż[7]. Ēśäņ×¼Ļ╣īņ¦ĆņØś ņåīņłśņØś ņ”ØļĪĆļ│┤Ļ│ĀņŚÉ ļö░ļź┤ļ®┤, ĒøäļæÉņØś ļ░śņĀäņä▒ ņ£ĀļæÉņóģņŚÉņä£ ļŗ©ĻĖ░Ļ░äņŚÉ ņ×¼ļ░£ņØĆ ĒÖĢņØĖļÉ£ ļ░ö ņŚåļŗż[4,11]. ĒøäļæÉņØś ļ░śņĀäņä▒ ņ£ĀļæÉņóģņŚÉ ļīĆĒĢ£ Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ ĻĖ░Ļ░äņØĆ ņĀĢļ”ĮļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖņ£╝ļéś ļ╣äĻ░Ģ ļé┤ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņŚÉ ņżĆĒĢśņŚ¼ Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ņØ┤ ĒĢäņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż.
ļ│Ė ņ”ØļĪĆļź╝ ĒåĄĒĢśņŚ¼, ĒøäļæÉ ņóģņ¢æņØś Ļ░Éļ│ä ņ¦äļŗ©ņŚÉ ļ░śņĀäņä▒ ņ£ĀļæÉņóģņØś Ļ░ĆļŖźņä▒ļÅä ļō£ļ¼╝ņ¦Ćļ¦ī Ļ│ĀļĀżĒĢśņŚ¼ņĢ╝ ĒĢ©ņØä ņĢī ņłś ņ׳ļŗż.