ņä£ļĪĀ
ņ£ĪņĢäņóģņØĆ ņāüņ▓ś ņ╣śņ£Ā Ļ│╝ņĀĢņŚÉņä£ ņāØĻĖĖ ņłś ņ׳ļŖö ņ¢æņä▒ ļ│æļ│ĆņØ┤ļŗż. ņØĖļæÉļéś ĒøäļæÉņŚÉ ļ░£ņāØĒĢśļŖö ņ£ĪņĢäņóģņØĆ ĻĘĖ ļ░£ņāØ ĻĖ░ņĀäņŚÉ ļīĆĒĢ┤ņä£ ņĢäņ¦ü ņØ┤Ļ▓¼ņØ┤ ņ׳ņ£╝ļéś[1], ņ£äņé░ņØś ņŚŁļźś[2-4], ĻĖ░Ļ┤ĆņéĮĻ┤Ć ļō▒ņØś ĻĖ░Ļ│äņĀüņØĖ ņåÉņāü[5,6], ņ£äņé░ņØś ņŚŁļźśņÖĆ ĻĖ░Ļ│äņĀü ņåÉņāüņØś Ēś╝ĒĢ®[7], ņØīņä▒ ļé©ņÜ®[4], Ēś╣ņØĆ ņØ┤ļ¼╝ņ¦ł ļ░śņØæ[8]Ļ│╝ ņŚ░Ļ┤ĆļÉśĻĖ░ļÅä ĒĢ£ļŗż. ņłśņłĀņĀü ņĀłņĀ£Ļ░Ć Ēæ£ņżĆņĀüņØĖ ņ╣śļŻīļ▓Ģ[5]ņØ┤ņ¦Ćļ¦ī ļåÆņØĆ ņ×¼ļ░£ļźĀ[9,10]ņØä ļ│┤ņØ┤ĻĖ░ļÅä ĒĢ£ļŗż.
ļ│Ė ņŚ░ĻĄ¼ņ×ÉļŖö ĻĄ¼ņØĖļæÉ Ēøäļ▓ĮņŚÉņä£ ĻĖ░ņŗ£ĒĢśņŚ¼ ņØĖļæÉ ņĀäņ▓┤ļź╝ ņ╣©ļ▓öĒĢśĻ│Ā ĒøäļæÉ ļ░Å ĻĖ░Ļ┤ĆĻ╣īņ¦Ć ņŚ░ņןļÉśņ¢┤ ļé┤ļĀżņÖĆ ņŚ░ĒĢśĻ│żļ×ĆņØä ņ┤łļלĒ¢łļŹś Ļ▒░ļīĆ ņ£ĪņĢäņóģ ņ”ØļĪĆļź╝ ļ│┤Ļ│ĀĒĢśļ®┤ņä£ ĻĘĖ ņøÉņØĖņŚÉ ļīĆĒĢ£ Ļ│Āņ░░ņØä ĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ņ”ØļĪĆ
50ņäĖ ņŚ¼ņ×ÉĻ░Ć ņŚ░ĒĢśĻ│żļ×ĆņØä ĒśĖņåīĒĢśļ®░ ļ│æņøÉņŚÉ ņÖöļŗż. ĒÖśņ×ÉļŖö 9Ļ░£ņøö ņĀä ļćīņČ£ĒśłļĪ£ ņłśņłĀņØä ļ░øņĢśĻ│Ā ņé¼ņ¦Ćļ¦łļ╣äļĪ£ ņ╣©ņāü ņāØĒÖ£ņØä ĒĢśĻ│Ā ņ׳ņŚłļŗż. ņØśņŗØņØĆ Ēś╝ļ»ĖĒĢ£ ņāüĒā£ļĪ£ ņØśņé¼ņåīĒåĄņØ┤ ņ¢┤ļĀżņøĀņ£╝ļ®░, ĻĖ░Ļ┤ĆņĀłĻ░£ņłĀņØä ļ░øĻ│Ā ĒŖ£ļĖīĻ░Ć ņéĮņ×ģļÉśņ¢┤ ņ׳ņŚłļŗż. ņ£äņĪ░ļŻ©(gastrostomy)ļź╝ ĒåĄĒĢśņŚ¼ ņŻ╝ļÉ£ ņśüņ¢æ Ļ│ĄĻĖēņØä ĒĢśļ®┤ņä£ ĻĄ¼Ļ░Ģ ņŗØņØ┤ļź╝ ņĪ░ĻĖłņö® ļ│æĒ¢ēĒĢśļŹś ĒÖśņ×ÉļĪ£, ĻĄ¼Ļ░Ģ ņŗØņØ┤Ļ░Ć ņĀäĒśĆ ņĢł ļÉśņ¢┤ ļ│Ė ļ│æņøÉņ£╝ļĪ£ ņĀäņøÉļÉśņŚłļŹś Ļ▓āņØ┤ļŗż.
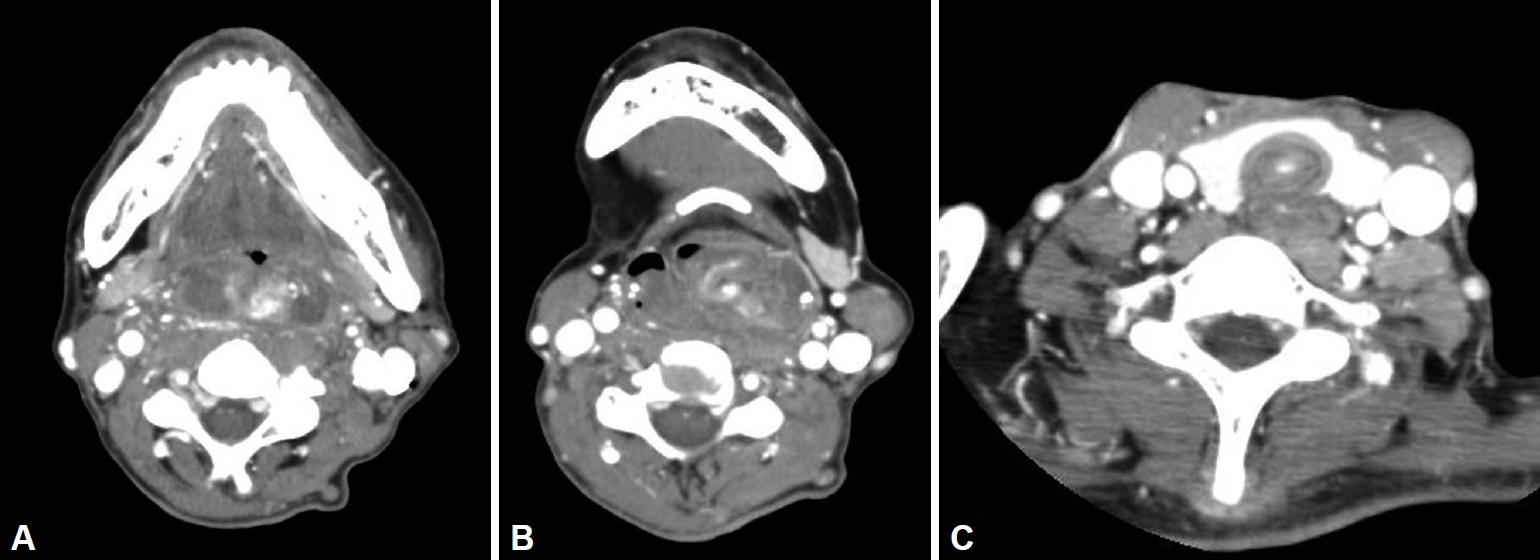
ņŗĀņ▓┤ Ļ▓Ćņé¼ņāü, ļ░▒ņāē Ēś╣ņØĆ ņśģņØĆ ļČäĒÖŹņāēņØś ļČĆļō£ļ¤ĮĻ│Ā ļ¦żļüłĒĢ£ Ēæ£ļ®┤ņØä Ļ░Ćņ¦ä ņŚ¼ļ¤¼ Ļ░£ņØś ņŚĮņØä Ļ░Ćņ¦ĆļŖö ļ»Ėļ¦īņä▒ ņ£ĪņĢäņä▒ ņóģļ¼╝ņØ┤ ĻĄ¼ņØĖļæÉ ņĀäņ▓┤ļź╝ ņĀÉņ£ĀĒĢśĻ│Ā ņ׳ņŚłļŗż(Fig. 1). ņØ┤ ļ│æļ│ĆņØĆ ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśüņāü ĻĄ¼ņØĖļæÉļ┐Éļ¦ī ņĢäļŗłļØ╝ ĒĢśņØĖļæÉļź╝ ĒżĒĢ©ĒĢ£ ņØĖļæÉ ņĀäņ▓┤ļź╝ ņ░©ņ¦ĆĒĢśļ®┤ņä£, ĒøäļæÉļź╝ ĒåĄĻ│╝ĒĢśņŚ¼ ĻĖ░Ļ┤ĆĻ╣īņ¦Ć ņŚ░ņןļÉśņ¢┤ ļé┤ļĀżņÖĆ ņ׳ņŚłļŗż(Fig. 2). ņ£ĪņĢłņĀüņØĖ Ļ┤Ćņ░░ņāü ņĀĆļ¬ģĒĢśĻ▓ī ļČĆļō£ļ¤¼ņÜ┤ ņ¢æņä▒ ļ│æļ│Ćņ£╝ļĪ£ ņāØĻ░üņØ┤ ļÉśņŚłĻ│Ā, ļśÉĒĢ£ Ē¢źĒøä ņ▓ĀņĀĆĒĢ£ ņĀ£Ļ▒░ ņłśņłĀņØä Ļ│äĒÜŹĒĢśĻ│Ā ņ׳ņŚłĻĖ░ņŚÉ ņłĀ ņĀä ņĪ░ņ¦üĻ▓Ćņé¼ļŖö ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņĢśļŗż.
ņĀäņŗĀļ¦łņĘ©ĒĢśņŚÉ ņłśņłĀņØä ņŗ£Ē¢ēĒĢśņśĆļŗż. ĒÖśņ×Éļź╝ ņĢÖņĢäņ£ä(supine position)ņŚÉņä£ Ļ░£ĻĄ¼ĻĖ░ļź╝ Ļ▒ĖĻ│Ā ĻĄ¼ņØĖļæÉļź╝ ļģĖņČ£ņŗ£ņ╝░ļŗż. ņóģļ¼╝ņØ┤ ĻĄ¼ņØĖļæÉņÖĆ ĒĢśņØĖļæÉ Ēøäļ▓ĮņØä ĻĘĀļō▒ĒĢśĻ▓ī ļ¬©ļæÉ ņ╣©ļ▓öĒ¢łņØä Ļ▓āņ£╝ļĪ£ ņśłņāüĒĢśņśĆņ£╝ļéś, ņśłņāüĻ│╝ ļŗ¼ļ”¼ ĒĢśņØĖļæÉņÖĆ ĒøäļæÉ ļ│æļ│ĆņØĆ ņŗżņĀ£ ņĀÉļ¦ēņØä ņ╣©ļ▓öĒĢśņ¦Ć ņĢŖĻ│Ā ĻĄ¼ņØĖļæÉ ņóģļ¼╝ņØ┤ ņĢäļלļĪ£ ļé┤ļĀżņśżļŖö ĒśĢĒā£(pedunculating)ņśĆļŗż.
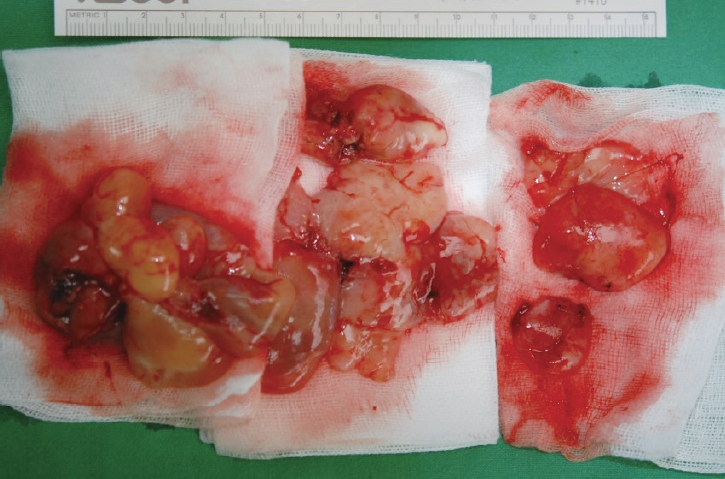
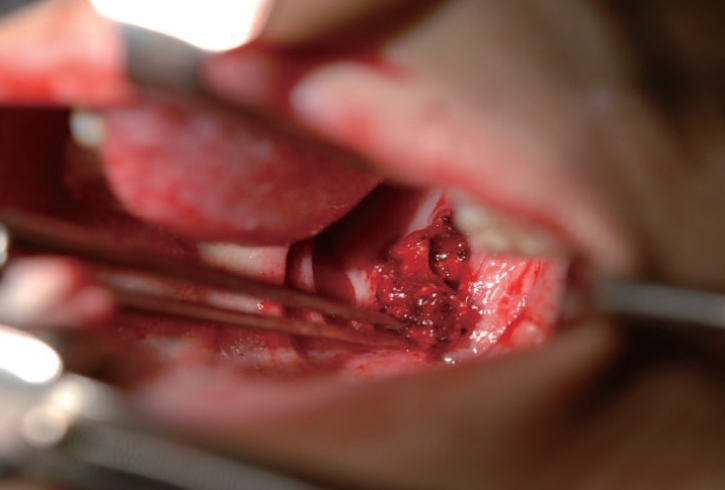
Ļ▓Ėņ×Éļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ĒøäļæÉ ļ░Å ĻĖ░Ļ┤ĆĻ│╝ ĒĢśņØĖļæÉļĪ£ ļé┤ļĀżņś© ņóģļ¼╝ņØä ļ¬©ļæÉ ņĀ£Ļ▒░ĒĢśĻ│Ā ĻĄ¼ņØĖļæÉ ņóģļ¼╝ņØś ļīĆļČĆļČäņØä ņĀ£Ļ▒░ĒĢśņśĆļŗż(Fig. 3). ĻĘĖļ¤░ļŹ░ ĻĄ¼ņØĖļæÉ ļČĆņ£äņŚÉņä£ļŖö ļīĆļČĆļČäņØś ņ£ĪņĢäņóģņØ┤ ņĀ£Ļ▒░ļÉ£ ĒøäņŚÉ ņØ╝ļČĆ ņĪ░ĻĘĖļ¦łĒĢ£ ņ£ĪņĢäņóģņØ┤ Ēøäļ▓ĮņŚÉ ļČÖņ¢┤ ņ׳ņ¢┤, ņØ┤ ļČĆņ£äĻ░Ć ņ£ĪņĢäņóģņØś ĻĖ░ņŗ£ ļČĆņ£äņ×äņØä ņČöņĀĢņ╝Ć ĒĢśņśĆļŗż. ĻĄ¼ņØĖļæÉ Ēøäļ▓ĮņØś ļé©ņØĆ ļČĆļō£ļ¤¼ņÜ┤ ņ£ĪņĢäņóģņØä ļ¬©ļæÉ ņĀ£Ļ▒░ĒĢśĻ│Ā Ļ┤Ćņ░░ĒĢ£ Ļ▓░Ļ│╝, ņĢĮ 2 cm ņĀĢļÅäņØś ņäĖļĪ£ ļ░®Ē¢źņØś ņĀÉļ¦ē Ļ▓░ņåÉ ļČĆņ£äĻ░Ć ņ׳ņŚłņ£╝ļ®░ ļö▒ļö▒ĒĢśĻ│Ā ņŻ╝ļ│Ć ņĪ░ņ¦üņ£╝ļĪ£ ņ£Āņ░®ļÉ£ ņä¼ņ£Ā ņĪ░ņ¦üņ£╝ļĪ£ ļ│ĆĒÖöļÉśņ¢┤ ņ׳ņŚłĻ│Ā, ņØ┤ ļČĆņ£äĻ░Ć ļ░öļĪ£ ņ£ĪņĢäņóģņØś ĻĖ░ņŗ£ļČĆņ×äņØä ņĢī ņłś ņ׳ņŚłļŗż(Fig. 4).
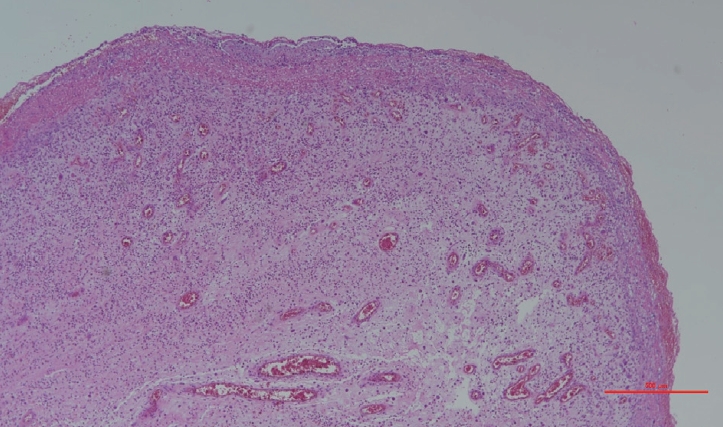
Ļ▓░ņåÉ ļČĆņ£ä ļ│æļ│ĆņØä ņĀäĻĖ░ņåīņ×æņłĀļĪ£ ņ▓ŁņåīĒĢśĻ│Ā ņ¢æņ¬Į ņĀÉļ¦ēņØä ļŗ╣Ļ▓© ņØ╝ņ░© ļ┤ēĒĢ®ņØä ņŗ£Ē¢ēĒĢśņśĆļŗż(Fig. 5). ņĀłņĀ£ļÉ£ ņóģļ¼╝ņØĆ ņĪ░ņ¦üĻ▓Ćņé¼ņāü ļ»ĖņäĖ ĒśłĻ┤ĆĻ│╝ ĒĢ©Ļ╗ś ņä¼ņ£ĀņĢäņäĖĒżņØś ņ”ØņŗØĻ│╝ ņŚ╝ņ”Øņä▒ ņäĖĒżņØś ņ╣©ņ£żņØä ļ│┤ņŚ¼ ņ£ĪņĢäņĪ░ņ¦üņ×äņØ┤ ĒÖĢņØĖļÉśņŚłļŗż(Fig. 6).
ĒÖśņ×ÉļŖö Ēć┤ņøÉ Ēøä 3ņŻ╝ ļ¦īņŚÉ ļ│æņøÉņŚÉ ļé┤ņøÉĒĢśņśĆņ£╝ļ®░, ņØ┤ ļĢī ņ£äņĪ░ļŻ©ļź╝ ĒåĄĒĢ£ ņśüņ¢æ Ļ│ĄĻĖēņØä ĒĢśĻ│Ā ņ׳ņŚłņ¦Ćļ¦ī ĻĄ¼Ļ░Ģņ£╝ļĪ£ļÅä ņŚ░ņŗØņØś ņŗØņØ┤ļź╝ ĒĢśĻ│Ā ņ׳ņŚłņ£╝ļ®░ ņŚ░ĒĢś Ļ│żļ×ĆņØ┤ļéś ĒØĪņØĖņØĆ ĒśĖņåīĒĢśņ¦Ć ņĢŖņĢśļŗż. ĒāłĻ┤Ć(decannulation)ņØä ĻČīņ£ĀĒĢśņśĆņ£╝ļéś, ņÜöņ¢æļ│æņøÉ ņØśļŻīņ¦äĻ│╝ ļ│┤ĒśĖņ×ÉĻ░Ć Ē¢źĒøä ĒÖśņ×É ņāüĒā£ņØś ņĢģĒÖö ļō▒ņØä ņŚ╝ļĀżĒĢśņŚ¼ ņ£Āņ¦ĆĒĢśĻĖ░ļĪ£ ĒĢśņśĆļŗż. 3Ļ░£ņøö ĒøäņØś ļé┤ņŗ£Ļ▓Į ņé¼ņ¦äņāü ņóģļ¼╝ņØś ņ×¼ļ░£ ņŚåņØ┤ ĻĄ¼ņØĖļæÉ Ēøäļ▓ĮņØ┤ ĒÜīļ│ĄļÉśņŚłņØīņØä ĒÖĢņØĖĒĢśņśĆļŗż(Fig. 7).
Ļ│Āņ░░
Shimazu ļō▒[11]ņØĆ 8ņŻ╝ ņŚ░ļĀ╣ņØś ņźÉņŚÉņä£ ņ£äņŗØļÅäņŚŁļźś ļ¬©ļŹĖņØä ļ¦īļōżņŚłļŗż. ņ”ē, ņ£äņØś ņ£Āļ¼Ė Ļ┤äņĢĮĻĘ╝(pyloric sphincter)ņØä ņÖĖļČĆņŚÉņä£ ļ¼ČĻ│Ā, ņĀäņ£ä(forestomach)ņÖĆ ņäĀ ļČĆņ£ä(glandular portion) ņé¼ņØ┤ņŚÉ ņ׳ļŖö ņØ┤Ē¢ē ļČĆņ£ä(transitional region)ļź╝ ņŗżļĪ£ ļ┤ēĒĢ®ĒĢśņŚ¼ ņ£äņé░ņØ┤ ņŗØļÅäļĪ£ ņŚŁļźśĒĢśĻ▓ī ļ¦īļōżņŚłļŗż. ĻĘĖļ¤░ļŹ░ ņØ┤ ļ¬©ļŹĖņŚÉņä£ ņ£äņé░ ņŚŁļźśņŚÉ ņØśĒĢ£ ĒøäļæÉ ņĀÉļ¦ēņØś ņŚ╝ņ”Ø ļ│ĆĒÖö(ņĀÉļ¦ēņØś ļ╣äĒøä, ĒśłĻ┤ĆņØś ņ”ØņŗØ ļ░Å ĒÖĢņן)ļŖö ņ׳ņŚłņ£╝ļéś 20ņŻ╝ ļÅÖņĢłņØś Ļ┤Ćņ░░ņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ņ£ĪņĢäņĪ░ņ¦üņØĆ ļ░£ņāØĒĢśņ¦Ć ņĢŖņĢśļŗżĻ│Ā ĒĢśņśĆļŗż.
ņØ┤ļōżņØĆ ņØ┤ ļ¬©ļŹĖņØä ļ░öĒāĢņ£╝ļĪ£ ļæÉ ļ▓łņ¦Ė ņŚ░ĻĄ¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŖöļŹ░[7], ņØ┤ļ▓łņŚÉļŖö ņźÉļź╝ ņ£äņŗØļÅäņŚŁļźśļź╝ ļ¦īļōĀ ĻĄ░Ļ│╝ ļīĆņĪ░ĻĄ░(ļ│ĄļČĆ ņżæņĢÖņĀłĻ░£ļ¦ī ņŗ£Ē¢ēĒĢ£ ĻĄ░), ļæÉ ĻĄ░ņ£╝ļĪ£ ļéśļłäĻ│Ā, ļ¬©ļōĀ ĻĄ░ņŚÉņä£ ĒöīļØ╝ņŖżĒŗ▒ ļ¦ēļīĆĻĖ░ļź╝ ĻĖ░Ļ┤Ć ņĢłņŚÉ ļäŻņØĆ Ēøä 3ņ┤łĻ░ä ņłśņ¦üņ£╝ļĪ£ ņäĖ ļ▓łņö® ņøĆņ¦üņŚ¼ņä£ ņä▒ļīĆ ņĀÉļ¦ēņŚÉ ņåÉņāüņØä ņŻ╝ņŚłļŗż. 2ņŻ╝Ļ░Ć ņ¦Ćļé£ Ēøä ļīĆņĪ░ĻĄ░ņŚÉņä£ļŖö ĒøäļæÉ ņĀÉļ¦ēņŚÉ ņ░░Ļ│╝ņāüĻ│╝ ņłśĒżļ¦ī Ļ┤Ćņ░░ļÉśņŚłņØä ļ┐É ņ£ĪņĢäņĪ░ņ¦üņØĆ ĒśĢņä▒ļÉśņ¦Ć ņĢŖņĢśņ£╝ļéś, ņ£äņŗØļÅäņŚŁļźśĻĄ░ņŚÉņä£ļŖö 60%ņØś ņźÉņŚÉņä£ ņ£ĪņĢäņĪ░ņ¦üņØ┤ Ļ┤Ćņ░░ļÉśņŚłĻ│Ā, ņØ┤Ļ▓āņØĆ ņé¼ļ×īņŚÉĻ▓īņä£ ļéśĒāĆļéśļŖö ņ£ĪņĢäņĪ░ņ¦üĻ│╝ ņĪ░ņ¦üĒĢÖņĀü ĒśĢĒā£Ļ░Ć ļ╣äņŖĘĒĢśņśĆļŗż.
ņØ┤ ļæÉ ņŗżĒŚś Ļ▓░Ļ│╝ļź╝ ĒåĀļīĆļĪ£ ņØ┤ļōżņØĆ ņ£äņé░ Ēś╣ņØĆ ĻĖ░Ļ│äņĀüņØĖ ņåÉņāü ļŗ©ļÅģņ£╝ļĪ£ļŖö ĒøäļæÉ ņĀÉļ¦ēņŚÉ ņ£ĪņĢäņĪ░ņ¦üņØä ĒśĢņä▒ņŗ£ĒéżĻĖ░ņŚÉ ņČ®ļČäĒĢśņ¦Ć ņĢŖņ£╝ļ®░, ņ£äņé░ ņŚŁļźśņÖĆ ĻĖ░Ļ│äņĀüņØĖ ņåÉņāüņØ┤ ļÅÖļ░śļÉśņŚłņØä ļĢī ņ£ĪņĢäņĪ░ņ¦üņØ┤ ĒśĢņä▒ļÉ£ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż.
ļ│Ė ņ”ØļĪĆņŚÉņä£ Ļ▒░ļīĆ ņ£ĪņĢäņĪ░ņ¦üņØ┤ ņØĖļæÉ Ēøäļ▓ĮņŚÉ ņāØĻĖ┤ ņØ┤ņ£Āļź╝ ņāØĻ░üĒĢ┤ ļ│┤Ļ│Āņ×É ĒĢ£ļŗż. Kim ļō▒[8]ņØ┤ ļ│┤Ļ│ĀĒĢ£ ļ░öņÖĆ Ļ░ÖņØ┤ Ļ▓ĮņČöņŚÉ Ļ│ĀņĀĢļÉ£ ĻĖłņåŹņŚÉ ļīĆĒĢ£ ņØ┤ļ¼╝ņ¦ł ļ░śņØæņŚÉ ņØśĒĢ£ Ļ▓āņØĆ ļ░░ņĀ£ĒĢĀ ņłś ņ׳ļŗż. ņØĖļæÉ Ēøäļ▓ĮņØ┤ ņ£ĪņĢäņĪ░ņ¦üņØś ĻĖ░ņŗ£ļČĆļØ╝ļŖö Ļ▓āņØä Ļ░ÉņĢłĒ¢łņØä ļĢī, ņ¢┤ļŖÉ ņł£Ļ░ä ņØ┤ ļČĆņ£ä ņĀÉļ¦ēņŚÉ ĻĖ░Ļ│äņĀüņØĖ ņåÉņāüņØ┤ ņ׳ņŚłņØä Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż. ļćīņČ£ĒśłĻ│╝ ņØ┤ļź╝ ņ╣śļŻīĒĢśļŖö Ļ│╝ņĀĢņŚÉņä£ ĻĖ░Ļ┤ĆņéĮĻ┤ĆņØ┤ļéś ļŗżļźĖ ņóģļźśņØś ņŗ£ņłĀ ļÅäņżæņŚÉņä£ ņØĖļæÉ ņĀÉļ¦ēņØ┤ ņåÉņāüļÉśņŚłņØä Ļ▓āņØ┤ļŗż. ĻĘĖļ”¼Ļ│Ā ņןĻĖ░Ļ░ä ņ╣©ņāü ņāØĒÖ£Ļ│╝ ļ╣äņ£äņśüņ¢æ(nasogastric) ĒŖ£ļĖī ņéĮņ×ģņ£╝ļĪ£ ņØĖĒĢ£ ņ£äņé░ ņŚŁļźśĻ░Ć ņ׳ņŚłņØä Ļ▓āņ£╝ļĪ£ ņČöņĀĢĒĢĀ ņłś ņ׳ļŗż. ļö░ļØ╝ņä£ ņØĖļæÉ Ēøäļ▓ĮņØś ņĀÉļ¦ē ņåÉņāüĻ│╝ ņ£äņé░ ņŚŁļźś ļæÉ Ļ░Ćņ¦Ć ņØĖņ×ÉĻ░Ć ļÅÖļ░śļÉśņ¢┤ ņŚ░ĒĢśĻ│żļ×ĆņØä ņ┤łļלĒĢśļŖö Ļ▒░ļīĆĒĢ£ ņ£ĪņĢäņĪ░ņ¦üņØ┤ ļ░£ņāØļÉśņŚłņØä Ļ▓āņ£╝ļĪ£ ņé¼ļŻīļÉ£ļŗż.
ļ│Ė ņ”ØļĪĆņ▓śļ¤╝ ņØĖļæÉ Ēøäļ▓ĮņŚÉ ņāØĻĖ┤ Ļ▒░ļīĆ ņ£ĪņĢäņóģņØĆ ļŗżļźĖ ļ¼ĖĒŚīņŚÉ ļ│┤Ļ│ĀļÉśņ¦Ć ņĢŖņØĆ ļ¦żņÜ░ ļō£ļ¼Ė Ļ▓ĮņÜ░ļĪ£ ĒīīņĢģļÉ£ļŗż. ņØ┤ņŚÉ ļ░śĒĢ┤ ņä▒ļīĆļÅīĻĖ░ ņ£ĪņĢäņóģņØĆ ņä▒ņØĖ ļé©ņ×ÉņŚÉĻ▓īņä£ ĒØöĒ׳ ļ░£ņāØĒĢśļŖö ņ¦łĒÖśņ£╝ļĪ£ ņŻ╝ļĪ£ ņ£äņŗØļÅäņŚŁļźś, ņéĮĻ┤Ć ņåÉņāü, ĻĘĖļ”¼Ļ│Ā ņØīņä▒ ļé©ņÜ®ņŚÉ ņØśĒĢ┤ ņāØĻĖ┤ļŗż. ņŻ╝ļĪ£ ļ░£ņä▒ņןņĢĀļź╝ ĒżĒĢ©ĒĢśņŚ¼ ļŗżļźĖ ņ”Øņāü, ņ”ē Ē׳ņŖżĒģīļ”¼ņä▒ ņ”Øņāü(globus symptom), ņĢĀņä▒, ĻĖ░ņ╣©, ņŚ░ĒĢśĒåĄ, ņØĖĒøäĒåĄņØä ņłśĻ░£ņøöņŚÉņä£ ņłśļģäņŚÉ Ļ▒Ėņ│É ĒśĖņåīĒĢ£ļŗż[9]. ĻĖ░Ļ┤ĆņéĮĻ┤Ć ĒøäņŚÉ ļ░£ņāØĒĢśļŖö Ļ▓ĮņÜ░ņŚÉļŖö ņä▒ņØĖ ņŚ¼ņä▒ņŚÉņä£ ĒØöĒĢśļ®░, ņØ╝ļ░śņĀüņØĖ ņ£ĪņĢäņóģĻ│╝ ļŗ¼ļ”¼ ĒŖ╣ņ¦ĢņĀüņ£╝ļĪ£ ņ╣śļŻī Ēøä ņל ņ×¼ļ░£ĒĢśņ¦Ć ņĢŖļŖöļŗż[12]. Ļ░Éļ│äĒĢ┤ņĢ╝ ĒĢĀ ņ¦łĒÖśņ£╝ļĪ£ļŖö ĒÄĖĒÅēņäĖĒżņĢö, ĒśłĻ┤Ćņóģ, ņ╣┤Ēżņŗ£ņ£Īņóģ, Ēś╣ņØĆ ĒśłĻ┤Ćņ£Īņóģ Ļ░ÖņØĆ ĒśłĻ┤Ćņä▒ ņ¦łĒÖś, ĒĢŁņāüĻĘĀ, ņ¦äĻĘĀ, Ēś╣ņØĆ ņé¼ļź┤ņĮöņØ┤ļÅäņ”Ø(sarcoidosis) Ļ░ÖņØĆ Ļ░ÉņŚ╝Ļ│╝ ņŚ░Ļ┤ĆļÉ£ ņŚ╝ņ”Ø ļ░śņØæņŚÉ ņØśĒĢ£ Ļ▓ĮņÜ░ ļō▒ņØ┤ļŗż[13,14].