ņä£ ļĪĀ
ņØśļŻī ĻĖ░ņłĀņØś ļ░£ņĀäĻ│╝ ļŗżņ¢æĒĢ£ ĒśĢĒā£ņØś ļĀłņØ┤ņĀĆņØś ļÅäņ×ģņ£╝ļĪ£ ĻĄŁņåīļ¦łņĘ© ĒĢś ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į ĒøäļæÉ ļĀłņØ┤ņĀĆ ņłśņłĀ(fiberoptic laryngeal laser surgery under local anesthesia, FLS)ņØś ņŚŁĒĢĀņØ┤ ņĀÉņ░© ņ”ØĻ░ĆĒĢśļŖö ņČöņäĖņØ┤ļŗż. ņØ┤ļŖö Ēśäņ×¼ņØś ņĄ£ņåī ņ╣©ņŖĄ ņłśņłĀ(minimal invasive surgery)ņØś ņŗ£ļīĆņĀü ĒØÉļ”äĻ│╝ ļ¦×Ļ│Ā ĻĖ░ņĪ┤ņØś ņĀäņŗĀļ¦łņĘ© ĒĢśņŚÉ ņŗ£Ē¢ēĒĢśļŖö ĒøäļæÉļ»ĖņäĖņłśņłĀ(laryngomicroscopic surgery, LMS)ņØś ņāüļŗ╣ ļČĆļČäņØä ļīĆņ▓┤ ĒĢĀ ņłś ņ׳ļŖö ļĢīļ¼ĖņØ┤ļŗż. ļö░ļØ╝ņä£ ĒøäļæÉņØīņä▒ņØśĒĢÖņØä ņĀäĻ│ĄĒĢ£ ņØśņé¼ļéś Ļ┤Ćņŗ¼ņØ┤ ņ׳ļŖö ņØ┤ļ╣äņØĖĒøäĻ│╝ ņØśņé¼ļŖö, ņČöĒøäņŚÉ ĻĘĖ ņŚŁĒĢĀņØ┤ ņĀÉņĀÉ ļåÆņĢäņ¦ł FLSņŚÉ Ļ┤Ćņŗ¼ņØä Ļ░ĆņĀĖņĢ╝ ĒĢĀ Ļ▓āņ£╝ļĪ£ ņé¼ļŻīļÉ£ļŗż.
ļ│Ė ļĪĀ
1. ĻĄŁņåīļ¦łņĘ© ĒĢś ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į ĒøäļæÉ ļĀłņØ┤ņĀĆ ņłśņłĀņŚÉ ņĀüņĀłĒÖś ĒÖśņ×ÉļŖö ņ¢┤ļ¢ż ĒÖśņ×ÉņØĖĻ░Ć?
ĻĖ░ļ│ĖņĀüņ£╝ļĪ£ FLSļŖö ĒøäļæÉļ»ĖņäĖņłśņłĀ(larryngoscopic microsurgery) ĒÖśņ×ÉļōżĻ│╝ ņĀüņØæņ”ØņØ┤ Ļ▓╣ņ╣śļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äņ£╝ļéś, ĻĄŁņåīĒĢśņĘ© ĒĢśņŚÉņä£ ņŗ£ņłĀĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ large sized lesionņØś Ļ▓ĮņÜ░ ĒÖśņ×ÉĻ░Ć Ēלļōżņ¢┤ĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äņ£╝ļ»ĆļĪ£, small to moderate sized benign vocal fold lesionņØ┤ ņóĆ ļŹö ņĀüņĀłĒĢśļŗż[1].
FLSļŖö ĻĄŁņåīļ¦łņĘ©ĒĢśņŚÉņä£ ņŗ£Ē¢ēĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ ĒÖśņ×ÉĻ░Ć gagĻ░Ć ņŗ¼ĒĢśĻ▒░ļéś, ļČłņĢłĒĢśĻ│Ā ņśłļ»╝ĒĢ£ ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ FLSļ│┤ļŗżļŖö ĻĖ░ņĪ┤ ĒøäļæÉļ»ĖņäĖņäĖņłĀ(conventional laryngomicroscopic surgery)Ļ░Ć ņČöņ▓£ļÉ£ļŗż. ļö░ļØ╝ņä£ ņłĀņĀäņŚÉņä£ ņÖĖļלņŚÉņä£ ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į(fiberscopy)ņØä ņŗ£Ē¢ēĒĢśļ®┤ņä£ ĒÖśņ×Éļź╝ ņäĀļ│äĒĢśļŖö Ļ▓āņØ┤ ņżæņÜöĒĢśļŗż[2].
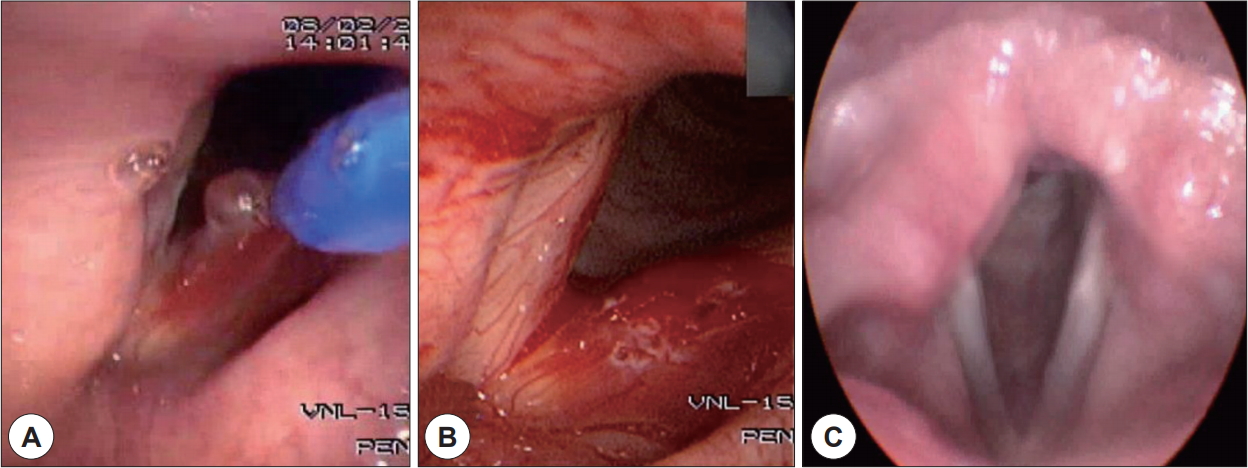
FLS ņłĀņŗØ ņ×Éņ▓┤ļĪ£ ņØśļ»Ė(unique value)Ļ░Ć ņ׳ļŖö Ļ▓ĮņÜ░ļŖö ĻĖ░ņĪ┤ ĒøäļæÉļ»ĖņäĖņłśņłĀ(laryngomicroscopic surgery)ļĪ£ ļģĖņČ£ņØ┤ ņ¢┤ļĀżņÜ┤ short neck, stiff neck, macrognathia, obesity, extension limitations of the cervical spine ļō▒ņØś difficult laryngeal exposure(DLE) ĒÖśņ×ÉņØĖ Ļ▓ĮņÜ░ņÖĆ ĒøäļæÉļ»ĖņäĖņłśņłĀ Ēøä ņŗ¼ĒĢśĻ▓ī ņĢŖĻ▓ī ņ×¼ļ░£ļÉ£(mild recurrence) ņä▒ļīĆ ņ¢æņä▒ļ│æļ│ĆņØś touch up procedureņØś Ļ▓ĮņÜ░ņØ┤ļŗż(Fig. 1) [3].
2. ĻĄŁņåīļ¦łņĘ©ĒĢś ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į ĒøäļæÉ ļĀłņØ┤ņĀĆ ņłśņłĀņØś ĻĄŁņåī ļ¦łņĘ© ļ░Å ļ¬©ļŗłĒä░ļ¦ü
ņĀĆņ×ÉņØś Ļ▓ĮņÜ░ FLSļź╝ ņŗ£Ē¢ēĒĢśĻĖ░ ļ░öļĪ£ ņĀäņŚÉ, Profopol 30 mg, Midazolam 3 mgļź╝ ĒÖśņ×ÉņŚÉĻ▓īņä£ ņĀĢļ¦ź ņŻ╝ņé¼ĒĢśņŚ¼ ĒÖśņ×Éļź╝ ņČ®ļČäĒ׳ ņ¦äņĀĢņŗ£Ēé© ļÆż, ņŗ¼ņĀäļÅä(EKG, electrocardiography), ņé░ņåīĒżĒÖöļÅä(pulse oxymetry)ļź╝ ņŗ£Ē¢ēĒĢśļ®┤ņä£ ĒÖśņ×Éļź╝ ļ¬©ļŗłĒä░ļ¦ü ĒĢśļ®┤ņä£ ņłśņłĀņØä ņ¦äĒ¢ēĒĢ£ļŗż[1].
ĒÖśņ×ÉņØś ĒøäļæÉļČĆņ£ä ļ¦łņĘ©ņØś Ļ▓ĮņÜ░, ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į(fiberscopy)ņØś side channelņØä ĒåĄĒĢśņŚ¼ 4% lidocaineņØä 2~3 mL ņĀĢļÅäņö® ļ┐īļ”¼Ļ▒░ļéś, Ēś╣ņØĆ side channelņØä ĒåĄĒĢśņŚ¼ spray catheterļź╝ ņé¼ņÜ®ĒĢśņŚ¼ ņŗ£Ē¢ēĒĢĀ ņłś ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī ļō£ļ¼╝Ļ▓ī ĒÖśņ×ÉņŚÉņä£ ļ”¼ļÅäņ╝ĆņØĖ ņć╝Ēü¼(lidocaine shock)ņØ┤ ļ░£ņāØĒĢĀ ņłś ņ׳ņ£╝ļ»ĆļĪ£, ņłĀņŗØ ņżæ ļ”¼ļÅäņ╝ĆņØĖ(lidocaine) ņĄ£ļīĆ ņÜ®ļ¤ēņØä 7~8 mL ņØ┤ĒĢśļĪ£ ņĀ£ĒĢ£ ĒĢśļŖö Ļ▓āņØ┤ ņČöņ▓£ļÉ£ļŗż. ņĀĆņ×ÉņØś Ļ░£ņØĖņĀü ņØśĻ▓¼ņ£╝ļĪ£ļŖö FLSĻ░Ć Ļ░ĆļŖźĒĢĀ ņĀĢļÅäņØś ņ░ĖņØäņä▒ņØ┤ ņ׳ļŖö ĒÖśņ×ÉņØś ņäĀĒāØĻ│╝, ņĀüņĀüĒĢ£ ĻĄŁņåīļ¦łņĘ©Ļ░Ć ņłĀņŗØņØś ņä▒Ļ│Ą ņŚ¼ļČĆļź╝ Ļ▓░ņĀĢĒĢśļŖö Ļ░Ćņן ņżæņÜöĒĢ£ ņÜöņØĖņØ┤ļŗż[4].
3. ĻĄŁņåīļ¦łņĘ©ĒĢś ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į ĒøäļæÉ ļĀłņØ┤ņĀĆ ņłśņłĀņØś ņןņĀÉ
FLSņØś Ļ░Ćņן Ēü░ ņןņĀÉņØĆ ņĀäņŗĀļ¦łņĘ©ļź╝ Ēö╝ĒĢĀ ņłś ņ׳ņ¢┤ņä£, Ļ┤ĆļĀ© ĒĢ®ļ│æņ”ØņØ┤ ņŚåĻ│Ā, ļ╣ĀļźĖ ĒÜīļ│ĄņØ┤ Ļ░ĆļŖźĒĢ£ ņןņĀÉņØ┤ ņ׳ļŗż. ļśÉĒĢ£ FLSņłĀņŗØ ņ×Éņ▓┤Ļ░Ć Ļ░äļŗ©ĒĢśĻ│Ā, ņłśņłĀ ņŗ£Ļ░äņØ┤ ņ¦¦Ļ│Ā, ĻĖ░ņłĀņĀüņ£╝ļĪ£ ņ¢┤ļĀĄņ¦Ć ņĢŖņØĆ ņןņĀÉņØ┤ ņ׳ļŗż[5].
ņØ┤ļ¤░ Ļ│╝ņĀĢņØä ĒåĄĒĢśņŚ¼ ņŗ£ņłĀņŚÉ ļīĆĒĢ£ ĒÖśņ×É ļ¦īņĪ▒ļÅäļź╝ ļåÆņØ╝ ņłś ņ׳ņ£╝ļ®░, ĻĖ░ņĪ┤ ĒøäļæÉļ»ĖņäĖņäĖņłĀ ņØ┤ ļČłĻ░ĆļŖźĒĢ£ difficult laryngeal exposure ĒÖśņ×ÉņÖĆ, ĻĖ░ņĪ┤ ĒøäļæÉļ»ĖņäĖņäĖņłĀ Ēøä ņ×¼ļ░£ĒĢ£ ņ¢æņä▒ ņä▒ļīĆļ│æļ│ĆņŚÉņä£ touch up procedure ļĪ£ņä£ Ļ│Āņ£ĀĻ░Ćņ╣ś(unique value)ļź╝ Ļ░Ćņ¦äļŗż[6].
ņĀĆņ×É Ļ░£ņØĖņĀüņ£╝ļĪ£ļŖö ņØīņä▒ ņÖĖĻ│╝ņØśļĪ£ņä£ ĻĖ░ņĪ┤ ĒøäļæÉļ»ĖņäĖņäĖņłĀņÖĖņŚÉ ļśÉ ĒĢśļéśņØś ņ╣śļŻī(treatment modality)ļź╝ Ļ░Ćņ¦ĆĻ▓ī ļÉ©ņ£╝ļĪ£ņŹ©, ĒÖśņ×ÉņŚÉĻ▓ī ņóĆļŹö ņĀüņĀłĒĢ£ ņ╣śļŻīĻ░Ć Ļ░ĆļŖźĒĢ£ ņןņĀÉņØ┤ ņ׳ļŗż.
4. ĻĄŁņåīļ¦łņĘ©ĒĢś ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į ĒøäļæÉ ļĀłņØ┤ņĀĆ ņłśņłĀņØś ņĀüņØæņ”Ø
FLSņØś ņ┤łĻĖ░ ņĀüņØæņ”Øņ£╝ļĪ£ ĒśłĻ┤Ćļ¦īņØä ĒŖ╣ņ¦ĢņĀüņ£╝ļĪ£ ņ╣śļŻīĒĢśļŖö(capillary targeted)ļŖö 532 nm ļĀłņØ┤ņĀĆņØś ņä▒ņ¦łņØä ņØ┤ņÜ®ĒĢśņŚ¼ hemorrhagic vocal polypņŚÉ ņ▓śņØī ļÅäņ×ģļÉśņŚłņ£╝ļ®░, ļśÉĒĢ£[7] ņä£ĻĄ¼ĻČīņŚÉ ņ£Āļ│æņ£©ņØ┤ ļåÆņØĆ ņ×¼ļ░£ņä▒ ĒøäļæÉņ£ĀļæÉņóģ(recurrent respirtory papillomatosis, RRP)ņŚÉ ĒÖĢļīĆ ņĀüņÜ®ļÉśņ¢┤ņä£ Ēśäņ×¼ļŖö Ēæ£ņżĆņ╣śļŻī ņ×Éļ”¼ņ×ĪņØĆ ņāüĒā£ņØ┤ļŗż[7].
5. ĻĄŁņåīļ¦łņĘ©ĒĢś ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į ĒøäļæÉ ļĀłņØ┤ņĀĆ ņłśņłĀņØś ļČĆņ×æņÜ® ļ░Å ņØ┤ņØś ņ▓śņ╣ś
ĻĄŁņåīļ¦łņĘ© ĒĢś ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į ĒøäļæÉ ļĀłņØ┤ņĀĆ ņłśņłĀņØś ļČĆņ×æņÜ®ņ£╝ļĪ£ļŖö ņĮöĒö╝(epistaxis), ļ»ĖņŻ╝ņŗĀĻ▓Į ņŗżņŗĀ(vasovagal syncope), ļ”¼ļÅäņ╝ĆņØĖņć╝Ēü¼(lidocaine shock), ĒøäļæÉĻ▓ĮļĀ©(laryngospasm) ņłśņłĀ ņóģĻ▓░ ņŗżĒī© ļō▒ ņØ┤ ļÉĀ ņłś ņ׳ļŗż
ņØ┤ ņżæ Ļ░Ćņן ĒØöĒĢ£ Ļ▓āņØĆ Ļ│╝ļÅäĒĢ£ gag reflex ļ░Å Ļ│╝ļÅäĒĢ£ ņä▒ļīĆ ņøĆņ¦üņ×ä ļō▒ņŚÉ ņØśĒĢ┤ ņłśņłĀņØä ņóģĻ▓░ĒĢĀ ņłś ņŚåļŖö Ļ▓ĮņÜ░ņØ┤ļŗż. ņØ┤ Ļ▓ĮņÜ░ ņ¢Ąņ¦ĆļĪ£ ĻĄŁņåīļ¦łņĘ©ļĪ£ ņłśņłĀņØä ņ¦äĒ¢ēĒĢśļŗżĻ░Ć ļ░£ņāØĒĢĀ ņłś ļČłņÖäņĀä ņłśņłĀ ļ░Å ņä▒ļīĆņåÉņāüņØä Ļ│ĀļĀżĒĢśņŚ¼, ņĀäņŗĀļ¦łņĘ©ĒĢśņŚÉ ĻĖ░ņĪ┤ ĒøäļæÉļ»ĖņäĖņäĖņłĀļĪ£ ņĀäĒÖśĒĢśļŖö Ļ▓āņØä ņĀĆņ×ÉļŖö ņČöņ▓£ĒĢ£ļŗż. ļ»ĖņŻ╝ņŗĀĻ▓Į ņŗżņŗĀņØĆ FLS procedure ņżæ ļ»ĖņŻ╝ņŗĀĻ▓ĮņØś Ļ░ĢĒĢ£ņ×ÉĻĘ╣(vagus nerve stimulation)ņŚÉ ņØśĒĢ┤ņä£ ļ░£ņāØĒĢśļ®░, ņ▓śņ╣śļŖö ņØ╝ļ░śņĀüņØĖ ņĀĆĒśłļ¤ēņć╝Ēü¼(hypovolemic shock)ņŚÉ ņżĆĒĢ┤ņä£ ņ╣śļŻīĒĢ£ļŗż[9].
ļō£ļ¼╝Ļ▓ī ļéśĒāĆļéśļŖö ļ”¼ļÅäņ╝ĆņØĖ ņĢäļéśĒĢäļØĮņŗ£ņŖż(lidocaine anaphylactic shock)ļŖö Ļ│╝ļÅäĒĢśĻ▓ī ļ¦ÄņØĆ ļ”¼ļÅäņ╝ĆņØĖņØä ļ¦ÄņØ┤ ĒøäļæÉņŚÉ ņĀÉņĀüĒĢśļŖö Ļ▓ĮņÜ░ļéś, lidocaineņŚÉ ļīĆĒĢ£ ĒÖśņ×ÉņØś Ļ│╝ļ»╝ļ░śņØæņŚÉ ņØśĒĢ┤ņä£ ļ░£ņāØĒĢśĻ▓ī ļÉ£ļŗż. ĒÖśņ×ÉļŖö ņØśņŗØņåīņŗż, Ļ▓ĮļĀ©, ĒśłņĢĢņĀĆĒĢś, dysrhythmia, ļō▒ņØś ņåīĻ▓¼, ņŗ¼ĒĢ£ Ļ▓ĮņÜ░ ĻĖ░ļÅäĒÅÉņćäļéś ĒøäļæÉĻ▓ĮļĀ©(laryngospasm) ņåīĻ▓¼ņØä ļ│┤ņØ╝ ņłś ņ׳ļŗż[10]. Anaphylactic shockņŚÉ ņżĆĒĢ┤ņä£ ņ╣śļŻīĒĢśļ®░, ĒŖ╣Ē׳ ĻĖ░ļÅäĒÅÉņćä ļ¼ĖņĀ£ ļ░Å ņŗ¼ņĀĢņ¦Ć(cardiac arrest) ļ░£ņāØņŗ£ ņØ┤ņŚÉ ļīĆĒĢ£ ņ▓śņ╣śĻ░Ć ĒĢäņÜöĒĢśļ®░, FLS ņŗ£ņłĀ ņżæ ļ░£ņāØĒĢĀ Ļ▓ĮņÜ░, ļ¦łņĘ©Ļ│╝ ņØśņé¼ņØś ļÅäņøĆņØä ļ░øņØĆ Ļ▓āņØ┤ ņČöņ▓£ļÉ£ļŗż
6. ĻĄŁņåīļ¦łņĘ© ĒĢś ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į ĒøäļæÉ ļĀłņØ┤ņĀĆ ņłśņłĀļ▓Ģ ļ░Å ņØ┤ņØś ņ×äņāü Ļ▓░Ļ│╝
2018ļģä Ēśäņ×¼ ĻĄŁļé┤ņŚÉņä£ ņĢłņĀäņä▒ņØ┤ ņ×ģņ”ØļÉ£ ĻĄ┤Ļ│ĪĒśĢ ļĀłņØ┤ņĀĆ(fiberoptic laser)ļĪ£ļŖö ņØ┤Ēāłļ”¼ņĢä Quanta System ņé¼ņØś ŌōćQunata 532 nm KTP laserņÖĆ ņØ┤ņŖżļØ╝ņŚś Luminis ņé¼ņØś ŌōćAcupulse Duo ļō▒ņØ┤ ņ׳ļŗż.
ņĢäņ¦ü ļ¼ĖĒŚīņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņ¦ä ņĢŖņĢśņ£╝ļéś ņĀĆņ×ÉļŖö ņ┤Ø 70ļ¬ģņØś ņä▒ļīĆĒÅ┤ļ”ĮĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ĻĄŁņåīļ¦łņĘ© ĒĢś ĻĄ┤Ļ│Īļé┤ņŗ£Ļ▓Į KTP ņä▒ļīĆļĀłņØ┤ņĀĆ(Qunata 532 nm KTP laser, Quanta System, Italy) ņłśņłĀņØä ņŗ£Ē¢ēĒĢśņŚ¼ 92.8% ĒÖśņ×ÉĻ░Ć(65/70ļ¬ģ) ĻĄŁņåīļ¦łņĘ© ĒĢś FLSļź╝ ņÖäļŻīĒĢĀ ņłś ņ׳ņŚłļŗż. ņłśņłĀ ņłĀĻĖ░ļŖö ņ×æņØĆ ļ│æļ│ĆņØś Ļ▓ĮņÜ░ ņĄ£ļīĆĒĢ£ ĻĘ╝ņĀæĒĢśņŚ¼ ļ│æļ│ĆņØä ļĀłņØ┤ņĀĆļĪ£ ņåīņ×æ(ablation)ņØä ĒĢśĻ│Ā, ņØ┤ ļ│┤ļŗż Ēü░ ļ│æļ│ĆņØś Ļ▓ĮņÜ░ ļĀłņØ┤ņĀĆļĪ£ ļ│æļ│ĆņØä ņåīņ×æĒĢśļ®┤ņä£ ļĀłņØ┤ņĀĆ ļüØņŚÉ ļ│æļ│ĆņØ┤ ļ¼╗ņ¢┤ļéśņśżĻ▓ī ĒĢśļŖö ļ░®ļ▓Ģņ£╝ļĪ£ ļ│æļ│ĆņØä ņĀ£Ļ▒░ ĒĢśņśĆļŗż(Fig. 2).
ņŗ£ņłĀ Ēøä 1Ļ░£ņøöņ¦ĖļČĆĒä░ Ļ▒░ņØś ļīĆļČĆļČäņØś ņŻ╝Ļ┤ĆņĀü, Ļ░ØĻ┤ĆņĀü ņØīņä▒ņ¦ĆĒæ£ļōżņØ┤ ņ£ĀņØśĒĢśĻ▓ī ĒśĖņĀäļÉśņŚłņ£╝ļ®░, ņØ┤ļŖö ņłĀ Ēøä 3Ļ░£ņøöĻ╣īņ¦Ć ņ£Āņ¦ĆļÉśļŖö ņåīĻ▓¼ņØä ļ│┤ņśĆļŗż(p’╝£0.05). ņłśņłĀ Ļ┤ĆļĀ© ĒĢ®ļ│æņ”ØļĪ£ļŖö 1ļĪĆ(1.4%)ņØś ņä▒ļīĆ Ēśłņóģ, 2ļĪĆ(2.8%)ņØś ļ”¼ļÅäņ╝ĆņØĖ ņć╝Ēü¼(lidocaine shock) ņåīĻ▓¼ņØä ļ│┤ņśĆņ£╝ļ®░, ņČöņĀü Ļ┤Ćņ░░ ĻĖ░Ļ░ä ņżæ 1ļĪĆ(1.4%)ņØś ņä▒ļīĆņ¦äļÅÖ Ļ░ÉņåīņÖĆ 2ļĪĆ(2.8%) ņä▒ļīĆĒÅ┤ļ”Į ņ×¼ļ░£ņåīĻ▓¼ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż.
Ļ▓░ ļĪĀ
ļĀłņØ┤ņĀĆ ĻĖ░ņłĀņØś ļ░£ņĀäĻ│╝ ņĀäņŗĀļ¦łņĘ©ļź╝ Ēö╝ĒĢśĻ│Āņ×É ĒĢśļŖö ņŗ£ļīĆņĀü ĒØÉļ”äņŚÉ ļ¦×ņČöņ¢┤, FLSĻ░Ć ņןņĀÉņØä Ļ░Ćņ¦ä ņłĀņŗØņØ┤ļéś, ļŗ©ņĀÉņŚåņØ┤ ņןņĀÉļ¦īņØä Ļ░Ćņ¦ä ņĀäĻ░ĆņØś ļ│┤ļÅäņÖĆ Ļ░ÖņØĆ ņłśņłĀļ▓ĢņØĆ ņĢäļŗłļŗż. ļĀłņØ┤ņĀĆļź╝ Ļ│╝ļÅäĒĢśĻ▓ī ņé¼ņÜ®ĒĢĀ Ļ▓ĮņÜ░ņŚÉļŖö ņä▒ļīĆņĪ░ņ¦üņŚÉ ļ╣äĻ░ĆņŚŁņĀü ņåÉņāüņ£╝ļĪ£ ņä▒ļīĆļ░śĒØöņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŗż. ļö░ļØ╝ņä£ ņłĀņ×ÉļŖö Ļ│╝ļÅäĒĢ£ ļĀłņØ┤ņĀĆ ņé¼ņÜ®ņŚÉ ļīĆĒĢ┤ņä£ Ļ▓ĮĻ│äņŗ¼ņØä Ļ░Ćņ¦Ćļ®┤ņä£, ņĀüņĀłĒĢ£ ĒÖśņ×ÉņŚÉĻ▓ī ņĀüņĀłĒĢśĻ▓ī ņé¼ņÜ®ĒĢśņśĆņØä Ļ▓ĮņÜ░ņŚÉ FLSĻ░Ć ņ£ĀņÜ®ĒĢ©ņØä ņØ┤ĒĢ┤ĒĢ┤ņĢ╝ ĒĢ£ļŗż.