국소 마취 하 굴곡 내시경 후두 레이저 수술로 치료한 성문 제자리 암종 1례
Abstract
The optimal treatments of carcinoma in situ of glottis include radiotherapy, laser surgery and vertical partial laryngectomy. Conventional surgical treatments need general anesthesia and radiotherapy has several complications. Recently, the effectiveness of 532 nm potassium titanyl phosphate (KTP) laser has been proven and widely used in vocal fold diseases even some cases of vocal fold dysplasia. A patient with difficult laryngeal exposure underwent fiberoptic laryngeal laser surgery using KTP laser under local anesthesia, showed improved voice outcome and the glottic lesion was removed successfully without local recurrence and regional metastasis 18 months after surgery.
Key words: Carcinoma in situ; Difficult laryngeal exposure; Fiberoptic laryngeal laser surgery
중심 단어: 굴곡 내시경 후두 레이저 수술; 성문 제자리 암종; 경부 신전 장애
서 론
기존의 경구강 후두미세수술(Transoral laryngomicrosurgery) 술식을 이용한 레이저 성대 절제술은 경부 신전이 어려운(Difficult laryngeal exposure, DLE) 환자에서 적용이 어려우며, 전신 마취 하 진행 되므로 고령이거나 기저 질환으로 인해 적용이 제한될 수 있다는 한계점이 있다[ 1]. 한편, 의료 기술의 발전과 더불어 개발된 국소 마취 하 굴곡내시경 후두 레이저 수술(Fiberoptic laryngeal laser surgery under local anesthesia, FLS)의 적응증이 확대되어 기존의 후두 양성 병변들 뿐만 아니라 성대 이형성증(Vocal fold dysplasia) 등에서 적용되어 좋은 결과를 보여주고 있다[ 2, 3]. 본 증례에서는 경부 신전이 어려운 환자에서 국소 마취 하 KTP 레이저를 이용한 굴곡내시경 후두 레이저 수술로 성문 제자리 암종(Carcinoma in situ of Glottis) 수술 후 재발 및 전이 소견 없이 성대의 기능을 유지하며 수술 후 18개월 째 추적관찰 중인 환자를 경험하여 이를 문헌과 함께 고찰하려 한다.
증 례
당뇨 및 폐결핵 과거력이 있는 71세 남성이 수개월간 지속된 목소리 변화를 주소로 타 병원 외래 내원하여 시행한 이학적 검사상 우측 성대 종물이 확인되었다. 해당 병원에서 전신마취 하 후두 미세 수술을 시도 하였으나 경부 신전 장애로 기관 삽관 시 어려움이 있었고, 병변 부위 노출이 불충분하여 종괴의 일부만 제거되었다. 조직 검사 결과 고도 형성이상(High grade dysplasia) 소견 보여 병변에 대한 추가 치료 위해 본원으로 의뢰되었다( Fig. 1, 2). 국소 마취 하 굴곡 내시경 후두 레이저 수술을 시행하기 위해 술 전 Midazolam 0.03~0.05 mg/kg을 정맥 주사하여 환자를 진정시키고, 1 : 100,000 Epinephrine, 1~2% Lidocaine 용액을 적신 거즈로 코 패킹을 하였다. 이후 굴곡 후두 내시경의 working channel을 이용하여 spray catheter를 통해 4% Lidocaine을 후두 부위에 분사하여 후두 부위를 국소 마취하였다. 굴곡 후두 내시경을 이용하여 병변을 확인하였고, 내시경의 working channel을 통해 KTP 레이저를 진입시켜 병변 주위 약 2 mm의 절제연을 두고 제거하였다( Fig. 3). 수술 후 시행한 조직 검사에서 중등도 분화도를 보이는 편평 상피 세포암(Moderately differentiated squamous cell carcinoma)으로 확인 되었다. 병리 조직학적 소견에서 T 병기는 제자리 암종(Carcinoma in situ)에 합당하여 추가적 방사선 치료 없이 추적 관찰 계획하였다.
수술 후 1개월 째 굴곡 내시경에서 우측 성대 수술 부위의 회복 양상을 보였다( Fig. 4). 수술 후 추적 관찰 위해 시행한 경부 자기 공명 영상 검사(MRI) 및 양전자 방출 단층 촬영 검사(PET-CT), 흉부 전산화 단층촬영 검사(Chest CT)에서 국소 전이 및 경부 림프절 전이의 증거는 없었다. 음성 분석 결과 술 전과 비교하였을 때, 주관적 음성평가 지표인 VHI(Voice handicap index) 30에서 수술 전 15점에서 수술 후 0점으로 명확한 주관적 호전을 보였다. 최대발성 지속시간(Mean phonation time)은 9.23초에서 술 후 3개월 째 11.45초로 증가하여, 정상 범위에 도달하였다. 음향분석검사에서 술 후 6개월 째 Jitter(0.87%→0.37%)와 Shimmer(5.49%→5.1%)는 향상되었다. 성대 점막 파동성(Mucosal wave)은 지속적으로 호전되었으며, 성문 폐쇄(Glottic closure) 또한 술 후 3개월 째에 완전히 회복되었다( Table 1)( Fig. 5). 수술 후 18개월 째 성대의 국소 재발 소견 보이지 않았으며, 성대 점막 파동성은 잘 유지되고 성문 폐쇄 또한 원활한 상태였다. 환자 목소리에 대한 주관적 만족도 높은 상태로 외래에서 추적 관찰 중에 있다( Fig. 6).
고 찰
성문 제자리 암종(Carcinoma in situ of glottis)은 조직학적으로 기저층(Basement membrane)을 침범하지 않으며 상피 전 층에 악성 세포가 보이는 전암성 병변(Premalignant lesion)으로, 여러 치료법이 논의 중에 있으나 방사선 치료, 수직 후두 부분 적출술(Vertical partial laryngectomy) 등이 주로 적용된다[ 4, 5]. 레이저 성대 절제술 또한 표준 치료로 자리 잡고 있으며, 최근 KTP 레이저(532 nm-potassium titanyl phosphate)는 다양한 후두 양성 질환에서 널리 사용되고 성대 이형성증에서도 적용되어 그 효용성이 입증된 바 있다[ 6, 7]. 레이저 성대 절제술에 주로 이용되어 온 CO 2 레이저는 주변 조직에 열 손상을 주고 성대에 반흔 조직을 만들 수 있으며, 굴곡형 내시경 하 CO 2 레이저를 사용할 경우 비용 부담의 단점이 있다. KTP 레이저의 532 nm 파장은 헤모글로빈에서 흡수되어 미세 혈관의 광 지혈 작용을 일으키는 원리로 종양의 신생 혈관(Tumor angiogenesis)을 막고, 에너지가 병변에 국한되는 특징이 있어 주변 정상 조직에 대한 손상을 최소화 하며, 적은 비용으로 굴곡형 내시경에 적용 가능하여 경제적으로 유리하다[ 8, 9]. 또한 기존 방사선 치료의 합병증인 구강 건조증, 경부 피부 자극, 삼킴 곤란 등이 발생하지 않는 장점이 있다. 전신 마취 하 후두 미세 수술 시 수술 시야의 확보는 레이저 수술의 시행 가능 여부를 결정하는 가장 중요한 요소 중 하나로, 환자의 목이 굵고 짧거나 입을 벌리기 힘든 경우, 경추경직으로 경부 신전이 안 되는 경우 등에서는 직접 후두경의 삽입이 힘들고 수술 시야가 확보되지 않아 레이저 성대 절제술이 매우 어려운 경우가 있다[ 10]. 본 증례에서는 경부 신전이 어려운 환자에서 국소 마취 하 굴곡 내시경 후두 레이저 수술을 시행함으로써 수술 시야를 충분히 확보하여 병변 전반에 대해 완전한 치료를 시행할 수 있었다. 또한 고령 및 당뇨 등 전신 질환으로 인해 전신 마취가 어려운 성문 제자리 암종 환자에서 기존의 방사선 치료나 수직 후두 부분 적출술의 대안으로 국소 마취 하 KTP 레이저를 이용한 굴곡 내시경 후두 레이저 수술을 시행하였다. 본 술식은 경부 신전 장애 및 기저 질환 등으로 인해 기존 치료법이 적용이 쉽지 않은 환자에 추천될 수 있으며, 소요 시간 및 경제적 측면에서도 수술적 부담이 적어 접근성을 높힌 방법으로서 성대 이형성증 또는 성문 제자리 암종 환자에서도 효과적인 치료 대안이 될 수 있을 것으로 사료된다. 추후 KTP 레이저 적용이 가능한 성문암 및 수술 이후 음성 보존 효과에 대한 지속적인 연구의 토대가 될 것이라는 것 또한 본 증례 보고의 의의라 하겠다.
Figure 1.
Preoperative laryngoscopic exam. Exophytic leukoplakic lesion with irregular surface on anterior portion of right vocal cord. 
Figure 2.
Lateral view of the patient with difficult laryngeal exposure. 
Figure 3.
Immediate postoperative laryngoscopic exam. KTP laser applied on right vocal cord. 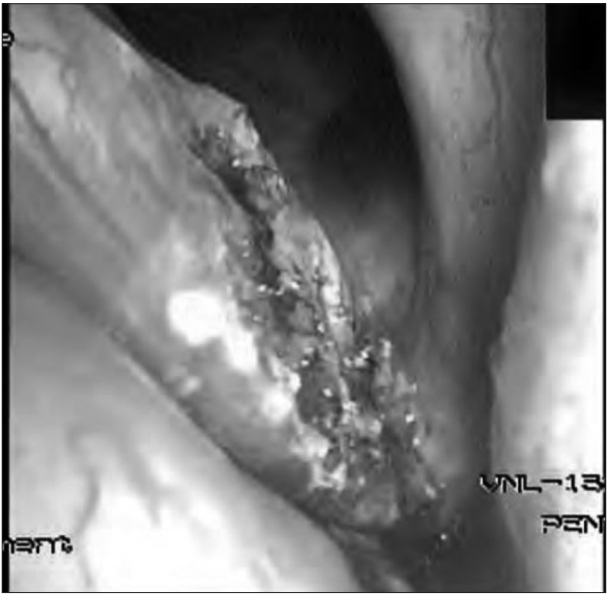
Figure 4.
Postoperative 1 month laryngoscopic exam. Healed surface of right vocal cord with mild swelling and no more leukoplakic lesion is seen. 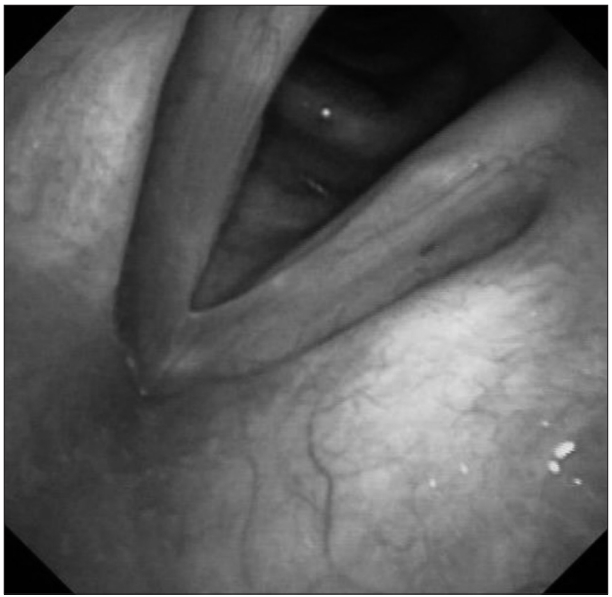
Figure 5.
Postoperative 6 months videostroboscopic exam. There was no glottic gap and both vocal cords moved symmetrically with normal mucosal wave. 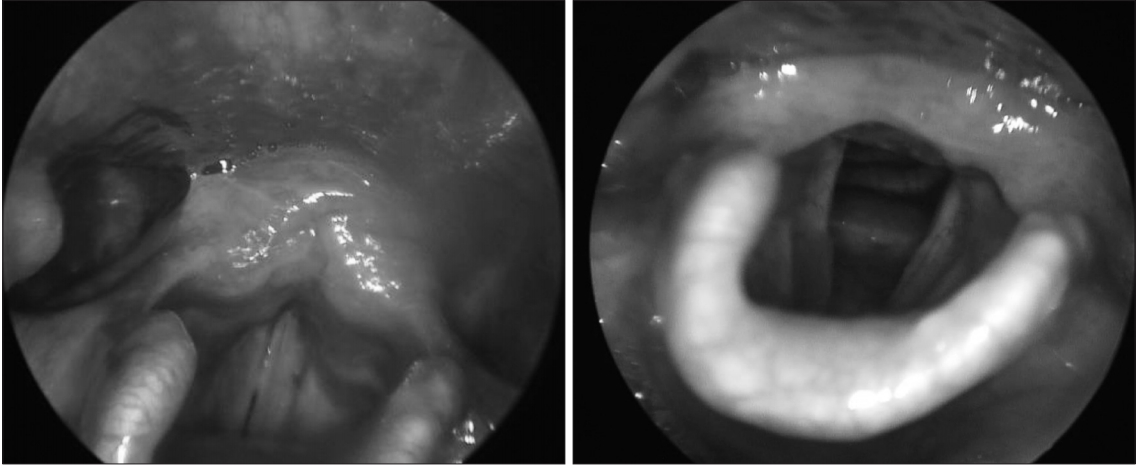
Figure 6.
Postoperative 18 months laryngoscopic exam. Gross finding of vocal cord was within normal range without any sign of local recurrence. Both subjective and objective evaluation of vocal cord function showed satisfying result. 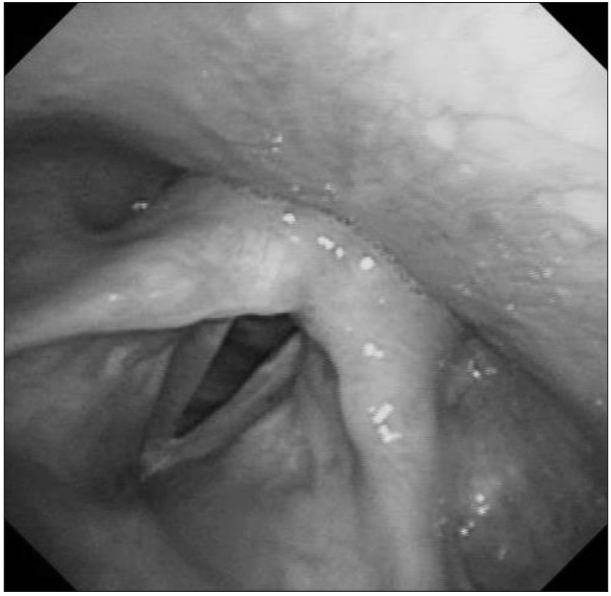
Table 1.
Preoperative and 3-month, 6-month postoperative voice parameters
|
VHI |
GRBAS |
MPT |
Jitter (%) |
Shimmer (%) |
NHR |
Mucosal wave |
Glottic closure |
|
Pre |
15 |
4 |
9.23 |
0.87 |
5.49 |
0.093 |
1 |
1 |
|
Post 3 M |
0 |
1 |
11.45 |
1.41 |
4.13 |
0.056 |
2 |
3 |
|
Post 6 M |
0 |
1 |
10.92 |
0.37 |
5.1 |
0.069 |
3 |
3 |
REFERENCES
1. Ohno S, Hirano S, Tateya I, Kojima T, Ito J. Management of vocal fold lesions in difficult laryngeal exposure patients in phonomicrosurgery. Auris Nasus Larynx 2011; 38( 3): 373- 80.   2. Xie X, Young J, Kost K, McGregor M. KTP 532 nm laser for laryngeal lesions. a systematic review. J Voice 2013; 27( 2): 245- 9. 3. Zeitels SM, Burns JA. Oncologic efficacy of angiolytic KTP laser treatment of early glottic cancer. Ann Otol Rhinol Laryngol 2014; 123( 12): 840- 6. 4. Le QT, Takamiya R, Shu HK, Smitt M, Singer M, Terris DJ, et al. Treatment results of carcinoma in situ of the glottis: an analysis of 82 cases. Arch Otolaryngol Head Neck Surg 2000; 126( 11): 1305- 12. 5. Park JH, Paeng JP, Na HS, Lim KJ, Kwon SY, Jung KY, et al. Treatment results of laser cordectomy and radiation therapy for early glottic cancer. Korean J Otolaryngol Head Neck Surg 2002;45(2):159-63.
6. Friedman AD, Hillman RE, Landau-Zemer T, Burns JA, Zeitels SM. Voice outcomes for photoangiolytic KTP laser treatment of early glottic cancer. Ann Otol Rhinol Laryngol 2013; 122( 3): 151- 8. 7. Zeitels SM, Burns JA, Lopez-Guerra G, Anderson RR, Hillman RE. Photoangiolytic laser treatment of early glottic cancer: a new management strategy. Ann Otol Rhinol Laryngol Suppl 2008; 199: 3- 24. 8. Hirano S, Yamashita M, Kitamura M, Takagita S. Photocoagulation of microvascular and hemorrhagic lesions of the vocal fold with the KTP laser. Ann Otol Rhinol Laryngol 2006; 115( 4): 253- 9. 9. Zeitels SM, Akst LM, Burns JA, Hillman RE, Broadhurst MS, Anderson RR. Office-based 532-nm pulsed KTP laser treatment of glottal papillomatosis and dysplasia. Ann Otol Rhinol Laryngol 2006; 115( 9): 679- 85. 10. Piazza C, Paderno A, Grazioli P, Del Bon F, Montalto N, Perotti P, et al. Laryngeal exposure and margin status in glottic cancer treated by transoral laser microsurgery. Laryngoscope 2018; 128( 5): 1146- 51.
|
|











