INTRODUCTION
Lobular capillary hemangioma (LCH) is a common vascular-proliferative tumor in the skin and oral mucosa, but rarely occurs in the larynx [1]. It was previously called pyogenic granuloma because it is reddish and nodular and is difficult to distinguish from laryngeal granuloma [2]. LCH is associated with trauma, pregnancy, and hormonal changes, but the cause has not been clearly identified [3]. It can occur in any age and sex group, but is predominant in young female adults, possibly due to hormonal effects on vessels [4]. LCH can cause various symptoms, such as hoarseness, throat discomfort, and dyspnea, as the mass grows [5]. We report the rare case of a 71-year-old female patient with LCH in the false vocal cord who was treated successfully without complications and briefly review the literature.
CASE REPORT
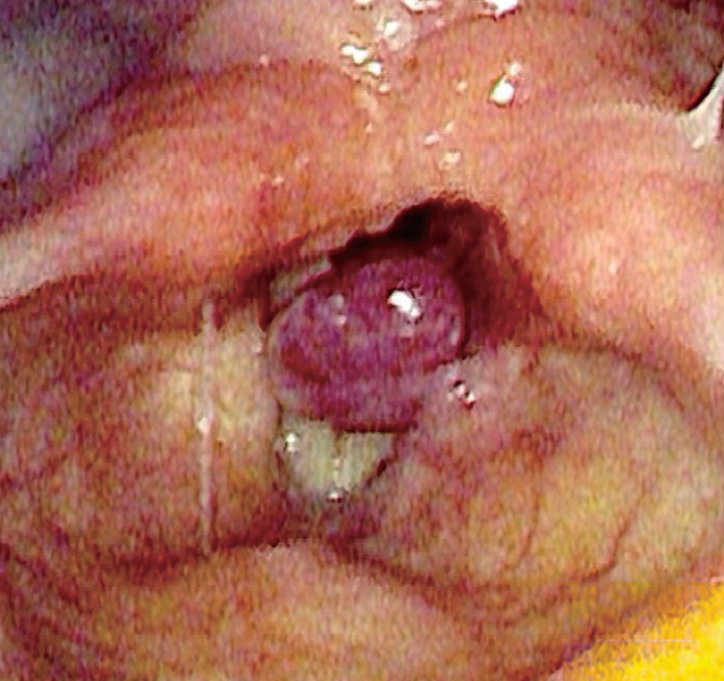
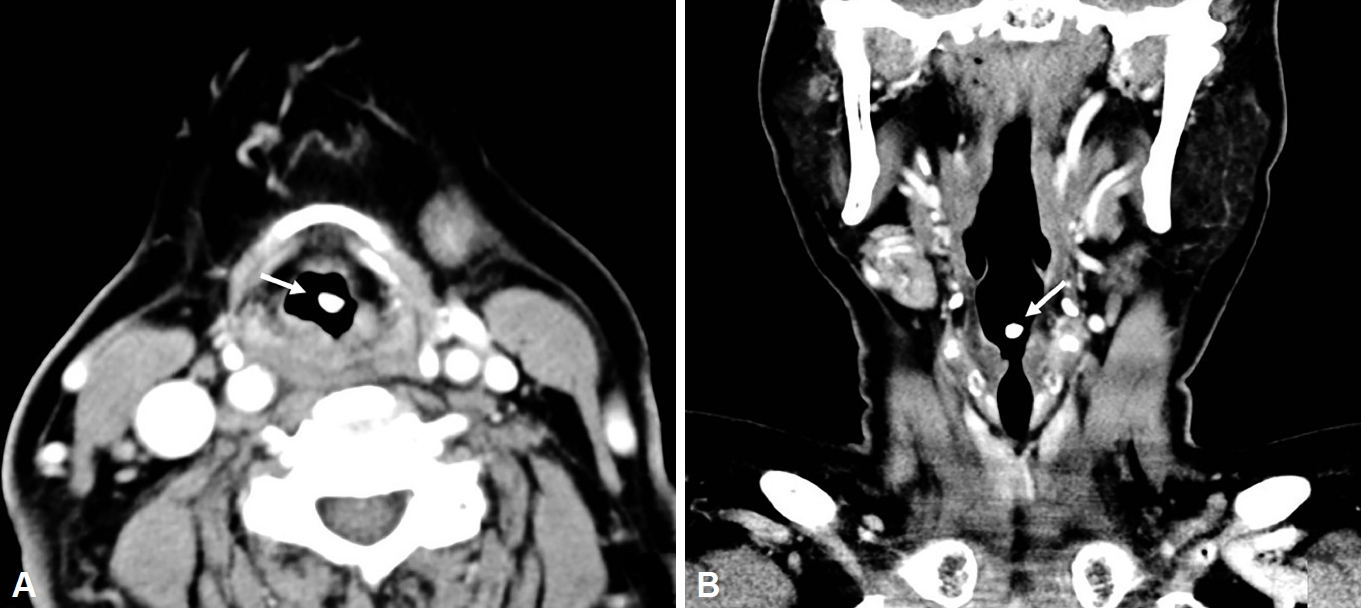
A 71-year-old female visited our clinic for throat discomfort, hoarseness, and intermittent stridor, which had lasted for 3 months. She did not complain of other symptoms such as cough, sputum, hemoptysis, and dyspnea. Her social history was unremarkable. She was a non-smoker and had no history of alcohol drinking. She also denied experience of voice abuse. She had twice received general anesthesia and received regular check-ups for essential hypertension. Laryngoscopic examination found a reddish, smooth surfaced, pedunculated, mass-like lesion at the left false vocal cord. Vocal cord motility was intact and aryepiglottic cartilage movement was clear (Fig. 1). Preoperative computed tomography revealed a well-enhanced, solid, and nodular tumor measuring 0.6 cm at the left false vocal cord (Fig. 2). We suspected it was a hemangioma or contact granuloma based on her medical history and endoscopic findings. The patient wished to undergo surgical removal; therefore, we planned to perform suspension laryngoscopic excision of the mass using a CO2 laser.
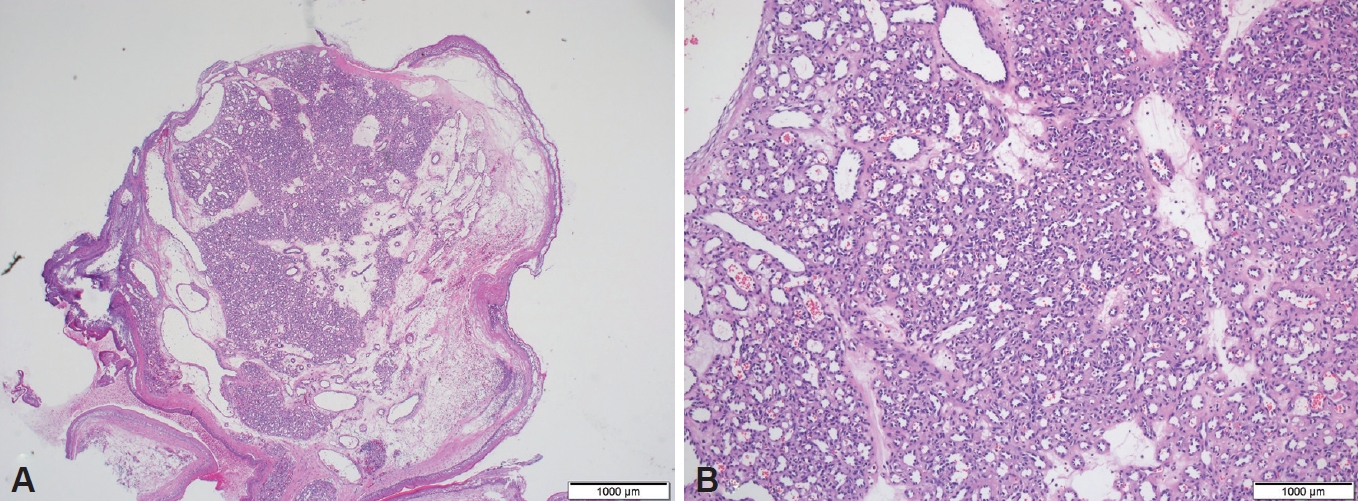
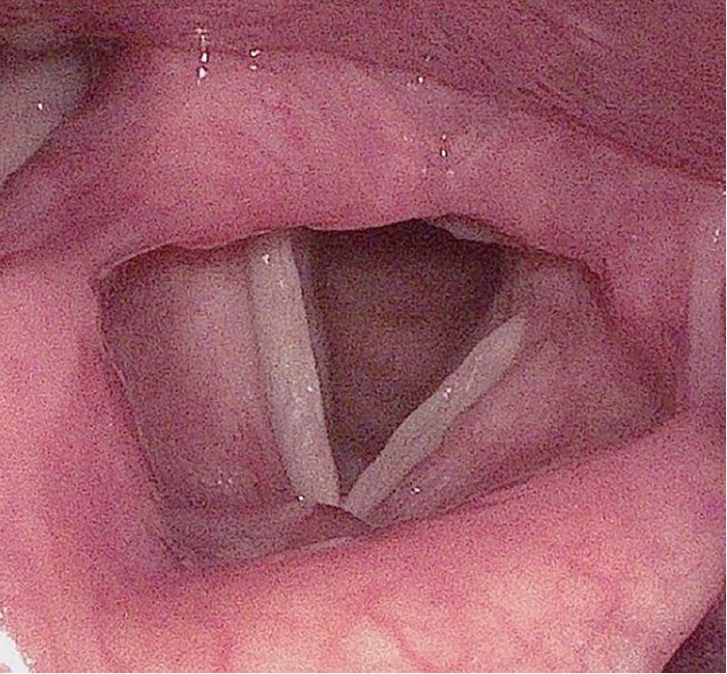
We carefully inserted a 5.5-cm-sized orotracheal intubation tube using video assisted technique to avoid disrupting the operation field. We prepared a CO2 laser, a suction bovie, and coagulation forceps to manage involuntary bleeding. The mass was pedunculated; therefore, we dissected the neck at the origin site using a CO2 laser set to continuous superpulse mode of 2 W. A vessel, suspected to be the feeding vessel, at the origin site was coagulated using coagulation forceps, and then the mass lesion was completely resected from the false vocal cord. There was no visible remarkable bleeding event or mucosal injury near the resection site. The mass was confined to the left false vocal cord. LCH was confirmed by pathology because the mass exhibited lobular formation of proliferative blood vessels of various sizes (Fig. 3). At 3 months after surgery, the patient is well and free of disease without any complaints (Fig. 4).
DISCUSSION
LCH, also known as pyogenic granuloma, is a benign vascular-proliferative tumor in the skin and oral mucosa [1]. The term ŌĆśpyogenic granulomaŌĆÖ is a pathologic misnomer because the lesion is not induced by bacterial infection and is not a granuloma. This term was introduced by Hartzell in 1904 [3]. In 1981, Fechner et al. [6] reviewed histological findings and corrected it to LCH because such masses show distinct lobular proliferation of capillaries rather than general granulomas.
Although the pathogenesis of LCH has not been clearly elucidated, it is believed to be related to trauma, hormonal changes, microscopic arteriovenous malformation, and effects of abnormal vascular endothelial growth factor [3]. Almost one-third of LCHs are located in the head and neck region [1]. It occurs frequently on the skin and oral mucosa, but rarely in the larynx (1%ŌĆō2%) [7]. Among LCH occurring in the larynx, it has been reported several times in the true vocal cords, which contact frequently due to vocalization, but has not previously been reported in the false vocal cord.
LCH is a dark red, pedunculated mass that is easily pressed. It is difficult to distinguish from a granuloma with the naked eye [3]. Symptoms can include throat discomfort and hoarseness depending on the location, size, and shape of the mass. Bleeding at the lesion can cause hemoptysis, and dyspnea is also possible if the lesion is large enough to block the airway. Management of LCH depends on the severity of symptoms [5]. If the lesion is small and does not cause symptoms, clinical observation is possible [4,8]. However, if the lesion causes symptoms and conservative therapy has no effect, surgical resection is the optimal treatment choice [2,4].
Complete surgical resection should be performed to prevent recurrence of LCH. Surgeons must prepare for massive bleeding, which can disrupt the operation field. After resection, aspiration or a large hematoma can occur in a short period of time; therefore, complete hemostasis and careful observation are required before the operation is completed.
We reported a LCH that could be mistaken for a granuloma in the larynx and briefly reviewed the literature.