INTRODUCTION
Foreign body (FB) aspiration into the tracheobronchial tree is a significant cause of morbidity and mortality in pediatric patients and continues to be a challenge for the otolaryngologist despite significant advances in prevention, first aid, and endoscopic technology [1,2]. The peak age of incidence is between 1 and 3-year-old and organic FB is more prevalent, dominated by peanuts [3]. Many organic FB can be aspirated at once [4], and one FB can be fragmented because the children can chew the food materials. For this reason, FB can be multiple and bilateral, however, bilateral bronchial FB is a rare condition and difficult to identify preoperatively and can be life-threatening if the complete FB retrieval is failed. Here, we present a case of a 20-month-old boy with bilateral bronchial FB which was successfully removed by endoscopy-assisted rigid bronchoscopy.
CASE REPORT
A 20-month-old boy with a 6-day history of FB aspiration was referred to our hospital for further evaluation. The FB was chewed walnut by history taking and he showed a wheezing sound with a mild cough. There was a wheezing sound with decreased breath sound on his left chest at physical examination.
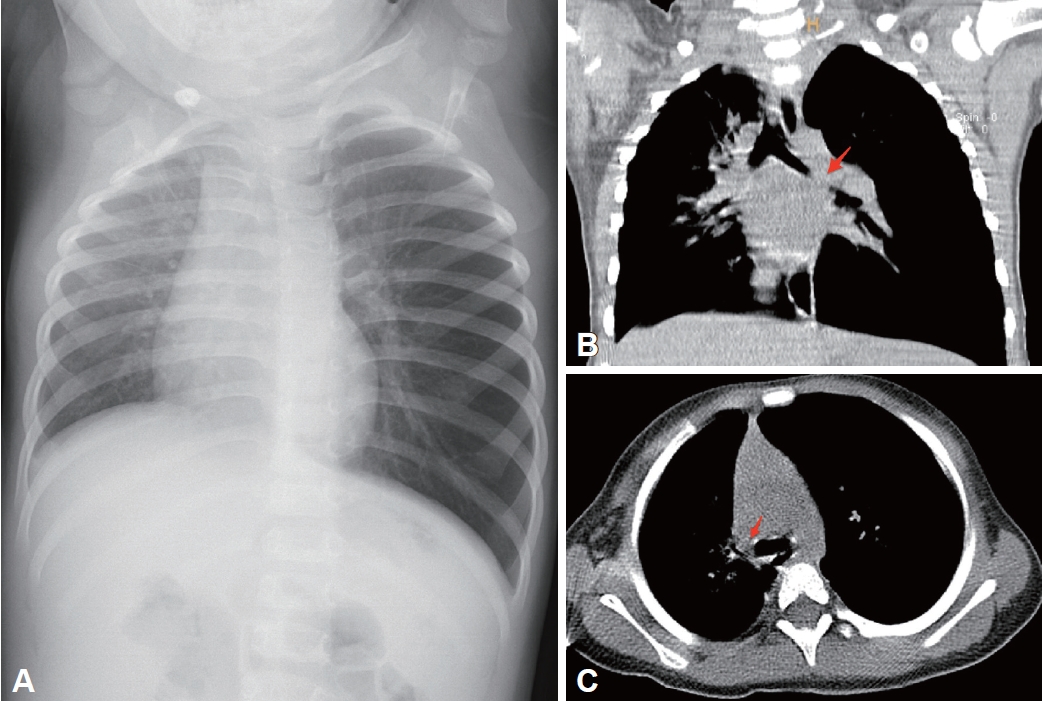
Chest radiography visualized hyperinflation of the left lung, displacement to the right side of the mediastinal structure, and atelectasis of the right upper lung zone (Fig. 1A). To determine the existence and location of the FB, low-dose chest CT was performed, and CT showed foreign material in the left main bronchus; the left main bronchus was almost completely occluded and the right main bronchus seemed to be not obstructive (Fig. 1B and C). A rigid bronchoscopic FB retrieval was requested for the retrieval of a FB.
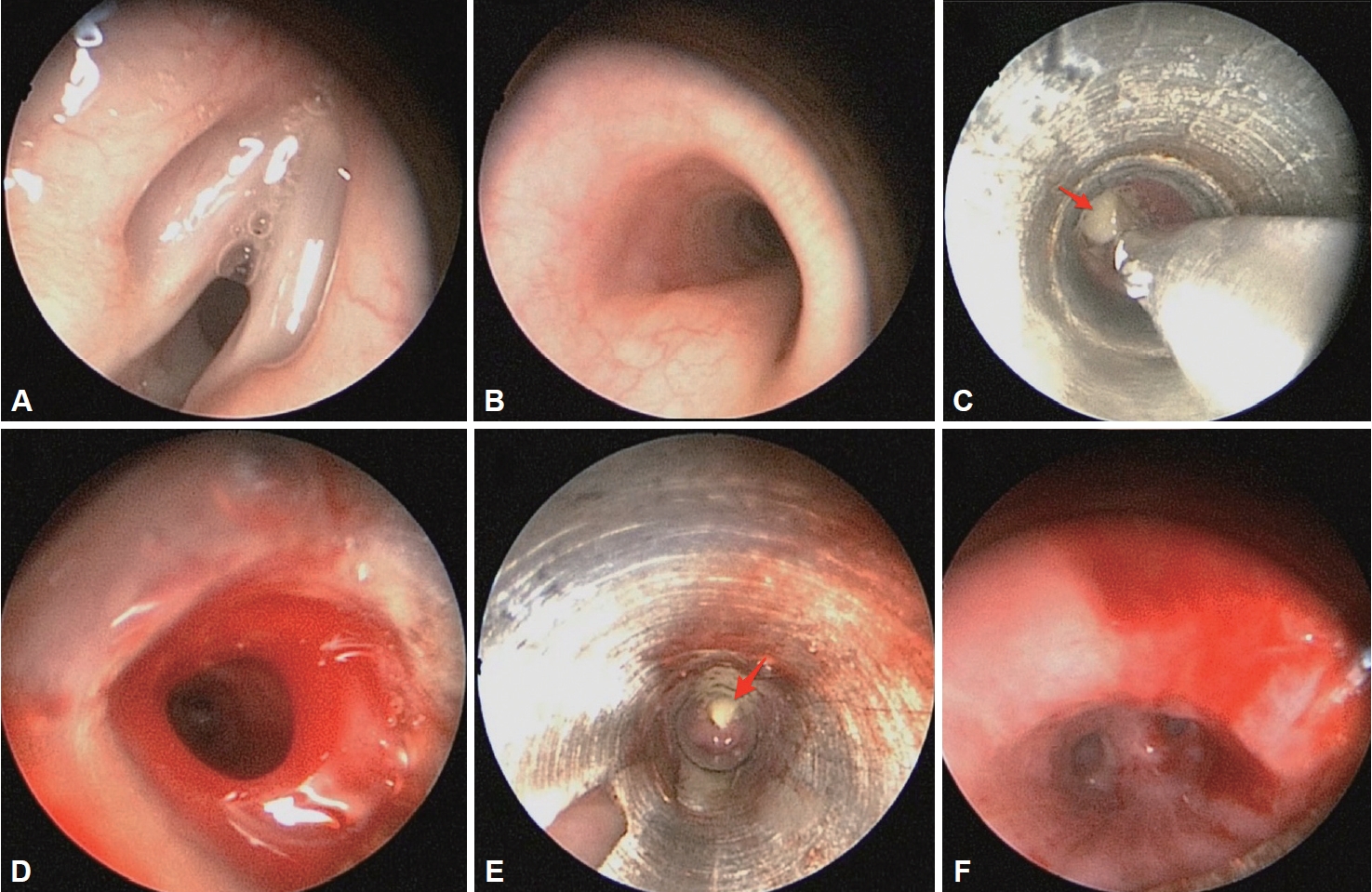
Under general anesthesia, rigid bronchoscopy (internal diameter 3.5 mm, Karl Storz GMBH & Co., Tuttlingen, Germany) with a 2.3 mm endoscope (Karl Storz GMBH & Co.) was intubated to the trachea (Fig. 2A and B). Under endoscopic guidance, bilateral bronchial FBs were separately identified which are lodged in the left main bronchus (size 6 mm) and right upper lobar bronchus (4 mm) (Fig. 2C and D). The FBs were successfully extracted by rigid forceps under endoscopy-assisted rigid bronchoscopy (Fig. 2C) and we confirmed that there was no remnant FB fragment in both bronchi (Fig. 2E and F) and recovery of the breath sound on both lungs.
The patient recovered well without any symptoms and signs of pulmonary complications and follow-up chest radiography showed no evidence of abnormal features (Fig. 3). He was discharged 4 days after the operation.
DISCUSSION
FB aspiration happens because children commonly have various objects or food in their mouth while playing, running, crying, laughing, or coughing, thus increasing the possibility of making a forced inspiring movement [5]. According to the literature and recent study, tracheobronchial FB was often unilateral and located in the right bronchial due to the anatomic angle, the right main bronchus being shorter and wider, as an extension of the trachea [3,6]. As we have seen in our case, it is a rare case of FBs that lodge in bilateral bronchi which was underdiagnosed preoperatively. Bilateral FB could be identified and removed because of our policy that the whole bronchial tree should be evaluated during bronchoscopic FB retrieval even though the patients with bilateral bronchial FBs tend to be desaturated quickly compared to unilateral FB patients.
The types of bronchial FB are variegated, depending on patient age and cultural background including religious beliefs as well as alimentary habits [7]. Bronchial FB can be multiple especially when children can chew the food materials and physicians should be concerned about the undetected FB which can be the cause of recovery delay after retrieval. Bilateral bronchial FB was reported at about 1.9% [3], and only one case was reported in Korean literature [8].
Chest radiography provides important information to the physician. The most common findings were mediastinum swing, emphysema, and atelectasis [9]. Common false-negative radiographs, however, cannot exclude the presence of FBs in the airways. In this instance, CT may help diagnose and in determining the exact existence and location of the FB in patients [10,11]. The chest radiography, in this case, visualized hyperinflation of the left lung, displacement to the right side of the mediastinal structure, and atelectasis of the right upper lung zone. The possibility of FB in the right upper bronchus was not concerned preoperatively because CT showed no definitive foreign material in the right bronchus. In this aspect, CT seems to be not helpful especially when FB is smaller than CT section thickness.
The removal of an FB can be performed with flexible or rigid bronchoscopy [12]. The selection of the endoscopic material depends on the physicianŌĆÖs preference. Some teams use flexible bronchoscope with the removal of substantially all FB, while most authors consider that rigid bronchoscope is a very safe and effective procedure in treating such patients [3]. We use a bimanual endoscope-assisted rigid bronchoscopy method which was reported as superior to the conventional naked eye method [13]. In addition, after FB removal, the patency of the tracheobronchial tree and remnant FB can be carefully examined with the magnified view by endoscopy-assisted rigid bronchoscopy. Our experience suggests that bilateral bronchi should be examined during bronchoscopic FB retrieval before and after surgery for conviction of remnant or undetected FB.