성문에서 발생한 재발성 흉선상 방추상 상피세포 종양(Spindle Epithelial Tumor with Thymus-Like Differentiation, SETTLE) 1예
A Case of Recurrent Spindle Cell Epithelial Tumor of Thymus-Like Differentiation (SETTLE) in the Glottis
Article information
Abstract
Spindle epithelial tumor with thymus-like differentiation (SETTLE) is an extremely rare type of thyroid tumor, with spares reports on its clinical course. SETTLE is derived from branchial pouch or thymic remnants, and classified as a low grade, malignant neoplasm due to its indolent growth and tendency to develop delayed metastasis. Therefore, stringent initial workups and long-term follow-up are required to prevent misdiagnosis. We present a case of recurrent spindle epithelial tumor with thymus-like differentiation (SETTLE) in the glottis of 57 year-old male patient, who had a history of surgical excision for the SETTLE from the thyroid gland 5 years ago. Transoral CO2 laser surgery was performed to remove the glottic tumor and there was no evidence of local recurrence at 11 months postoperatively.
서 론
흉선상 방추상 상피세포 종양(Spindle epithelial tumor with thymus-like differentiation, SETTLE)은 갑상선과 경부에 드물게 발생하는 종양으로, 1991년 Chan과 Rosai에 의해 처음으로 소개되어, 2015년까지 총 42례가 보고된 바 있는 악성 종양이다[1,2].
SETTLE은 발생학적으로 제3 및 제 4 인두낭 이나 잔존 흉선으로부터 기원하여 초기 흉선의 분화(primitive thymic differentiation) 양상을 보인다고 알려져 있으며, 대부분 소아나 젊은 층에서 발생한다. 조직학적으로 이상성 종양(biphasic tumor)으로, 방추 세포(spindle cell)와 상피 세포(epithelial cell)로 구성된 치밀한 배열을 보이는데, 방추세포 또는 상피세포 단일 분화로 이루어 지기도 한다[3].
SETTLE로 진단된 경우 수술적으로 제거하는 것이 일반적이며, 호발 하는 부위인 갑상선의 한쪽 엽에 국한되면, 일측 갑상선 엽절제술을 하거나, 종양만 제거해도 안전하다는 보고가 있다[4]. SETTLE은 성장이 느린 종양으로 수술적 제거가 가능한 경우, 치료 성공율이 높고, 대부분 예후가 좋은 편으로 알려져 있으나, 일부 뒤늦게 임파선 혹은 혈관성 전이를 하는 악성 종양의 특성을 보인다는 보고도 있어서 수술 후 장기간의 경과 관찰이 필요하다[2,3,5].
전이는 주로 경부 임파선, 폐, 종격동에 나타나는 것으로 알려져 있으며, 그 외 신장이나 뼈에 전이한 사례도 보고된 바 있다[4]. 전이가 발견된 경우 외부 방사선치료나 항암화학치료를 시행하기도 하나 증례가 많지 않아서 아직 정립된 치료법은 없다[2,3].
저자들은, 갑상선에서 발생한 SETTLE 제거술 후, 성문에 국소 재발성으로 발견된 SETTLE을 수술적으로 치료한 경험을 보고하고자 한다.
증 례
57세 남자는 5년 전 외부 병원에서 좌측 갑상선을 침범하는 8.2 cm 크기의 종물에 대해 갑상선 전 절제술을 시행 받았으며(Fig. 1A), 당시 조직검사 소견은 흉선상 방추상 상피세포 종양(Spindle epithelial tumor with thymus-like differentiation)으로 나왔다. 이후 추가 치료 없이 이학적 검사 및 경부 컴퓨터 단층촬영을 주기적으로 실시하며 경과 관찰하던 중, 내원 8개월 전 시행한 양전자 방출 컴퓨터 단층촬영(PET-CT) 및 흉부 전산화 단층 촬영 상 다양한 크기의 다발성 결절이 양측 폐에 관찰되어, 폐 전이를 배제할 수 없으나 크기가 작아서 추가적인 조직검사 없이 경과관찰을 하고 있었다.

Representative images of computed tomography (CT). A : Initial CT scan shows huge thyroid mass with homogeneous attenuation (white arrows). Note the close contact between mass and the thyroid cartilage. There is no evidence of mass lesion at the glottis. B : Preoperative CT scan shows 1.1×1.0 cm sized, enhancing mass involving anterior commissure and bilateral vocal cord (white arrow). There is no evidence of local recurrence at thyroidectomy site. C : Follow-up CT scan at 6months postoperatively demonstrates no recurrent tumor at the larynx (white arrow). D : Follow-up Chest CT presents multiple lung nodules at bilateral lobes with no interval change of size and characteristics (white arrows).
환자는, 처음 갑상선 수술 이후 목소리 변화를 느꼈으며, 이후 호전되지 않고 쉰 목소리가 점점 심해지는 양상을 보여, 이에 대한 상담 위해 내원하였으며, 당시 시행한 이학적 검사상 양측 성대의 운동성은 정상이었으나, 성대의 전연합부(anterior commissure)에 유두상 종물이 관찰되었다(Fig. 2). 이에 시행한 후두부 컴퓨터 단층촬영 상, 전연합부와 양측 성대 전방을 침범하면서 조영증강을 보이는 종물이 관찰되어, 원발 성문암과 SETTLE의 전이암에 대한 감별진단이 필요하였다, 이전에 수술한 갑상선 부위와 양측 경부에는 특이 소견이 없었다(Fig. 1B). 진단 목적으로 전신마취 하에, 현수후두경 하에서 종양을 절개 생검 하였으며, 동결절편검사에서는 점막 하에 비정형적 원형세포(atypical small round cells) 정도만 확인되며 명확한 감별진단이 어려웠고, 이후 최종 병리조직검사 상, 이전 원발 종양 조직 검사 결과와 같은 SETTLE로 진단되었다(Fig. 3). 추가로 시행한 면역화학검사상 CK(AE1/AE3), CD99, P63에서 양성, EMA, TLE-1, TTF-1 등은 음성이었다.
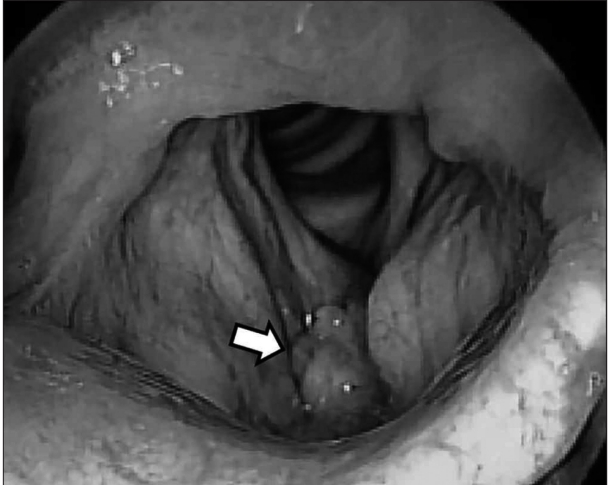
Laryngoscopic image. Preoperative endoscopic finding revealed exophytic, papillomatous mass occupying the anterior commissure and true vocal cords.
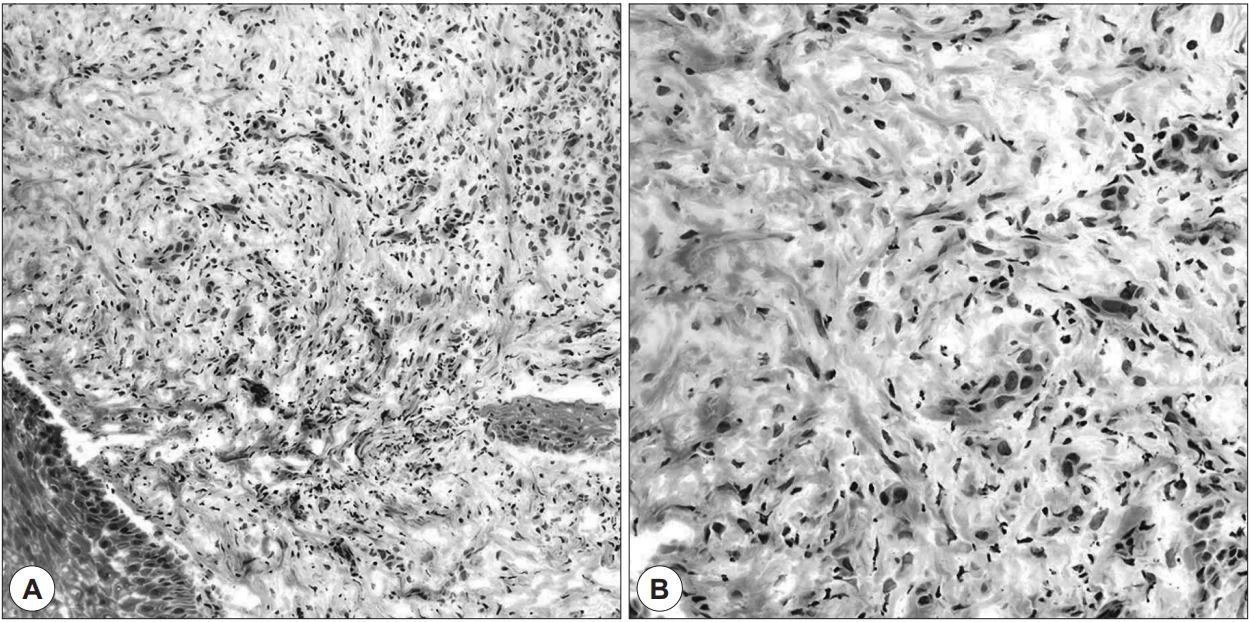
Rathologic images. Spindle epithelial tumor with thymus-like differentiation (SETTLE) from the glottis. A : Biphasic tumor with compact arrangement of spindle cells and epithelial cells (H & E, ×200). B : Spindle-shaped epithelial cells which have a sharp interface with the stroma, elongated nuclei with delicate chromatin and inconspicuous nucleoli, and little cytoplasm (H & E, ×400).
조직 검사 결과에 따라 잔여 종양의 제거를 위해, 다시 전연합부에서 성문하까지 CO2 레이저를 이용한 성문절제술 type I을 시행하였고, 수술 중 내시경으로 잔여 종양이 없음을 확인하였다. 동결절편검사 및 최종 병리조직검사 결과에서도 절제연이 확보된 소견이였다. 수술 후, 추가적인 항암치료나 방사선 치료 없이, 경과관찰 하고 있으며, 수술 후 11개월 째 시행한 후두부 컴퓨터 단층촬영에서는 재발 종양은 보이지 않았으며(Fig. 1C), 후두 내시경에서는 전연합부의 경한 유착이 보였으나, 쉰 목소리는 호전되었다. 추적 흉부컴퓨터 단층촬영에서 폐결절의 크기는 변화가 없는 상태로, 추가적인 항암화학요법 없이 경과관찰 중이다(Fig. 1D).
고 찰
SETTLE은 갑상선에 발생하는 저 위험 악성 종양으로, 발생 빈도가 드물어, 문헌 고찰 상 지금까지 42례가 보고되어 있다. SETTLE은 조직학적으로 흉선과 유사하지만, 기존에 보고된 41례의 원발 종양은 갑상선에 위치하고 있었으며, 나머지 1례에서는 원발 위치가 기술되어 있지 않았다[2]. 임상적으로 뚜렷하게 나타나는 증상은 없으나[6], 주로 무통성의 비대칭적인 경부 혹은 갑상선 종물을 주소로 내원하게 되는 경우가 많으며, 드물게 종양의 직접적인 침범으로 인한 호흡곤란 및 통증이 있는 경우도 있었다[1,3,7]. 요오드 신티그라피에서도 조영 증강 소견을 보이지 않으며, 갑상선 기능검사에도 이상소견이 없는 특징을 보인다[2,3]. 세침흡인세포검사는 다른 질환을 배제하기 위해서 시행되며, SETTLE의 의심은 가능하나 갑상선 수질암과 감별을 요하며, 정확한 진단을 위해서는 병리조직검사가 필요하다[5,8]. 병리 소견 상, 긴 방추형의 세포와 선상구조가 같이 나타나는 것이 특징으로, 타원형 형태의 핵을 Heamtoxylin & Eosin(H&E) 염색으로 쉽게 관찰할 수 있다. 갑상선 실질이나 주위 연부 조직에 침윤되어 있는 양상을 띠며, 세포의 유사분열 활동이나 괴사는 잘 관찰되지 않는다[8,9]. 방추상 세포와 상피 세포가 혼합되어 나타나기 때문에 병리학적으로는 윤활막 육종(synovial sarcoma)과의 감별을 요하기도 한다[9].
SETTLE은 수술적 절제가 치료의 근간을 이루며, 수술 후 완벽하게 제거하지 못한 잔존 종양이 있거나, 전이하는 경우에는 추가 절제 및 방사선 치료, 또는 항암화학치료가 시행되기도 한다. 보고된 증례의 26%의 환자에서 원격 전이가 있었으며, 혈관이나 림프관을 통해 폐와 종격동에 가장 흔하게 전이를 일으켰으며, 간, 신장 등 다양한 부위의 전이도 보고된 바 있다. 국소 재발 및 원격 전이가 발생하는 기간은 수술적 절제로부터, 짧게는 2개월, 길게는 22년까지 발생 기간의 차이가 있고, 대개 전이가 일어나기까지의 잠재 기간(latency)이 긴 편이다[2,5,8]. 원격 전이가 일어난 경우에는 최근까지 보고된 11명 중 4명이 사망하였다[2]. 하지만, 관찰 기간이 짧은 경우도 있어, 원격 전이 발생률 및 사망률이 저평가 되었을 가능성이 높다. 전이된 경우에도 수술적 치료가 가능한 경우에는 절제 후 좋은 결과를 얻었고, 그렇지 않은 경우, 방사선 치료나 항암화학치료를 고려하게 되는데 증례가 많지 않아 적절한 치료제나 치료기간은 정립된 바가 없다. 항암치료는 주로 cisplatin, etoposide, cyclophosphamide, ifosfamide 등이 사용되었고, 완전 관해가 보고된 바 있다[11]. 이전 보고에서는 전이 종양에 대한 수술적 치료는 폐, 신장, 골 전이에서 시행된 바가 있으며, 절제 후 좋은 결과를 얻었다[8,10,12].
본 증례에서는 갑상선에 발생한 SETTLE의 수술적 절제 후, 성문에 같은 조직학적 종양이 발생하였는데, 1) 최초 갑상선 수술 직후부터 목소리 이상을 호소하였고, 2) 처음 시행한 영상검사 상, 갑상선 종양이 갑상연골과 경계가 구별되지 않을 정도의 유착 내지 침범소견이 보였다는 점을 고려해 볼 때, 성문부에 발생한 SETTLE은 전신전이보다는 갑상선 종양의 인접부위 국소 재발 소견으로 보는 것이 타당하다고 생각된다. 또한, 성문부 종양 수술 후 11개월 간 경과 관찰하여, 다소 기간이 짧아 향후 장기적인 추적 관찰을 통해, 국소 재발 및 폐 전이의 진행 여부를 확인해야 할 필요성이 있다.
본 증례는 기존에 SETTLE이 경부 림프절 전이 및 폐나 복부장기에 원격전이가 있었던 것과는 다른 양상으로 주목할 필요가 있다. SETTLE은 비록 발생빈도는 낮고, 아직까지 재발률 및 재발 시 예후가 불명확하며, 치료법에 대한 정립된 바가 없어, 수술 전 전신 병기에 대한 정확한 진단과 함께, 수술 후 장기적 추적관찰이 매우 중요하다. 특히, 초치료 후 5년이 지난 후에도 전이가 발생하는 경우가 보고되어 있어, 다른 종양에 비하여 긴 추적 관찰 기간이 필요하다. 저자들은, 성문부 SETTLE에 대한 치료 경험과 함께 문헌고찰을 통한 전반적인 진단, 치료 및 추적 관찰에 대해 보고하는 바이다.