건상검진상 발견된 Killian-Jamieson Diverticulum 1예
A Case of Killian-Jamieson Diverticulum in the Esophagus
Article information
Trans Abstract
A Killian-Jamieson diverticulum (KJD) is an unfamillar and unusual cervical esophageal diverticulum. This diverticulum originates on the anterolateral aspect of the esophagus through the Killian-Jamieson’s area that is formed between cricopharyngeal muscle and the lateral to longitudinal esophageal muscle. Recently, we experienced a patient who was found outpouching lesion on lateral side of left esophagus on the duodenoscopy. Then, a barium esophagography performed and in left lateral position demonstrated a left-sided diverticulum with a frontal projection, highly suggestive of a KJD. There are two ways of surgical approach to manage the KJD. First is external approach, another one is endoscopic approach. In common, external approach has been recommended for the treatment of KJD because of concern of nerve injury. We present a case of KJD that underwent external approach and sternocleidomastoid muscle flap in the management of KJD.
서 론
식도의 게실은 해부학적 발생위치에 따라 크게 2가지로 나눠 볼 수가 있다. 가장 흔한 형태는 Zenker’s diverticulum (ZD)으로 식도의 하부괄약근과 윤상인두근 사이에서 발생하여 식도의 후방으로 발생하게 된다. 이와는 달리 식도의 뒷부분이 아닌 앞부분으로 형성되는 게실이 존재하는데 Killian-Jamieson diverticulum(KJD)이 여기에 해당된다. KJD는 1983년에 Ekberg와 Nylander에 의해 처음 소개된 게실로서 윤상인두근과 식도종주근 사이의 취약한 지점인 Killian-Jamieson triangle에서 발생하게 된다[1]. KJD의 진단은 바륨을 이용한 식도조영검사를 통해 이루어지게 되며 조영된 영상에서 보이는 게실의 위치로 게실의 종류를 구분하게 된다[2].
증상을 호소하는 게실 환자의 경우 수술적 치료를 진행하게 되는데 KJD의 수술적 치료에는 크게 2가지 방법이 있다. 첫번째는 경부절제술로 외부에서 접근하는 방법이고, 두번째는 내시경을 이용하여 구강내로 접근하는 방법이다. 최근들어 내시경을 이용한 수술이 많이 진행되고 있으나 이는 되돌이 후두신경 손상의 위험성이 있다[2].
본 환자는 증상을 호소하는 게실환자로서 경부절개를 통한 수술을 진행하였으며 게실을 찾아서 절제한 후 재발을 막기 위해 윤상인두근 절제술을 시행하였고 게실을 제거한 부위의 강화를 위해 목빗근회전피판술을 시행한 환자이다.
증 례
47세 남자, 경부 이물감 및 경부의 불편감을 호소하던 환자로, 특별한 내과적 병력은 없었다.
건강검진을 위해 시행한 위내시경상 비입구로부터 약 20 cm 떨어진 식도 좌측에서 게실이 발견되었다(Fig. 1). 정확한 진단을 위해 바륨울 이용한 식도조영검사를 시행하였고 식도 좌측과 앞쪽으로 형성된 게실 주머니를 확인할 수 있었다(Fig. 2). 그밖에 인두 후두 및 식도에 이상 소견은 보이지 않았다.
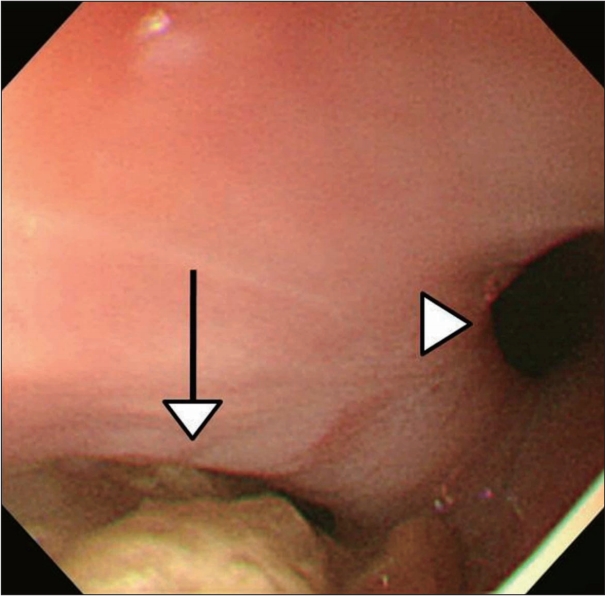
In the endoscopic image, diverticulum is located in the left side of esophagus (white arrow). Esophagus is also seen (white arrow head).
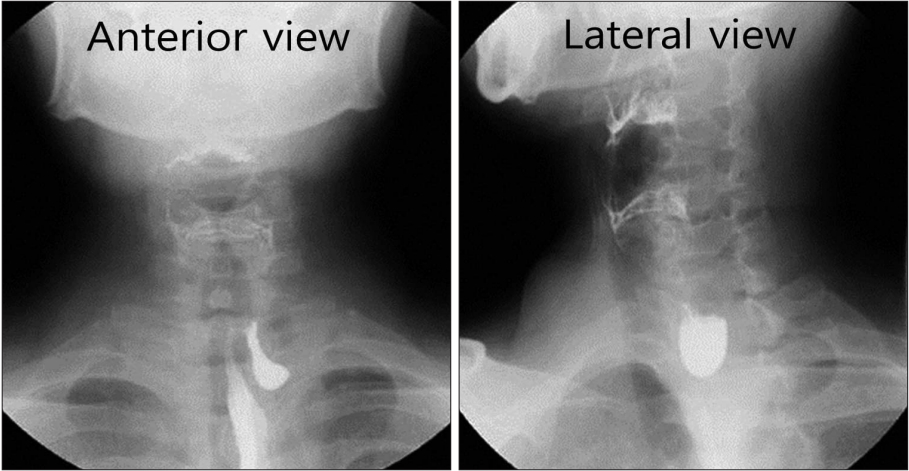
In esophagography, outpouching sac is seen on the left anterior aspect of esophagus in the anterior view and lateral view.
식도조영검사에서 게실이 형성된 위치 및 방향으로 미루어 KJD로 진단하였고 증상을 호소하는 게실환자에 대한 수술적 치료를 계획하였다. 수술 전 경부전산화단층촬영 시행하였고 식도좌측으로 형성되어있는 크기 약 2.7 cm의 게실 주머니를 확인하였다(Fig. 3).

In Computed tomography scans, 2.7 cm length outpouching sac is located on the left lateral wall of cervical esophagus.
전신마취하에 게실절제술을 시행하였고 처음에는 내시경적 접근을 시도하였으나 게실까지의 접근이 용이하지 않았고 되돌이 후두신경의 손상 가능성이 우려되어 경부절개를 통하여 수술을 진행하였다.
환자는 먼저 경부 좌측의 큰 주름을 따라서 절개를 한 후 좌측 목빗근을 바깥쪽으로 당겨주고 견장근육을 안쪽으로 당겨주었다(Fig. 4A). 그 후 게실을 찾기 위해 경부탐색을 시행하였고 게실 및 되돌이 후두신경을 확인하였다. 게실은 Endo-GIA 45 mm purple stapler를 이용하여 절제하였고(Fig. 4B) 절제 후 게실의 재발방지를 위해 윤상인대 절제술을 바로 시행하였다(Fig. 4C). 이후 게실제거부위의 강화를 위한 목빗근회전피판술을 시행하였다(Fig. 4D).
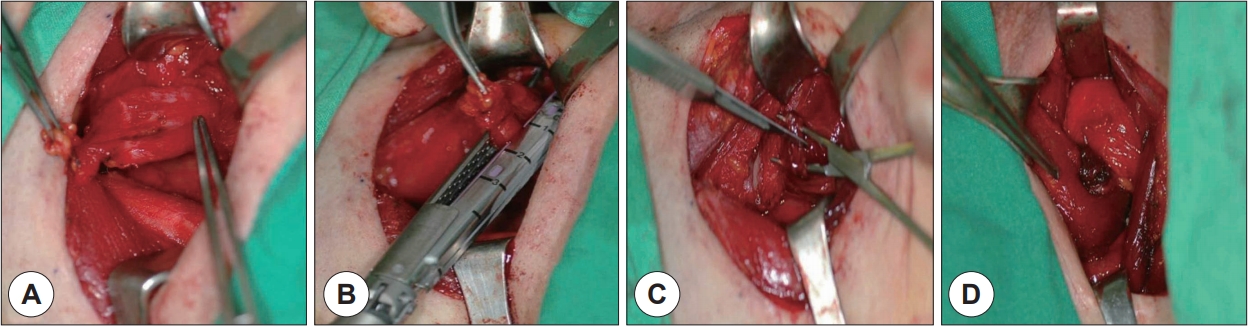
After incision was done, sternocleidomastoid muscle was retracted laterally, strap muscle was retracted medially (A). Recurrent laryngeal nerve and Killian-Jamieson diverticulum was found and diverticulum was cut by Endo GIATM stapler #45 mm purple (B). And then cricopharyngeal muscle myotomy was done (C). Sternocleidomastoid muscle rotation flap was done (D).
수술 후 1주일 째 수술 부위의 누출을 확인하기 위해 식도조영술을 시행하였고 조영제 누출이나 누공 소견 보이지 않아(Fig. 5) 일반식이 진행 후 술 후 10일 째 퇴원하였다.
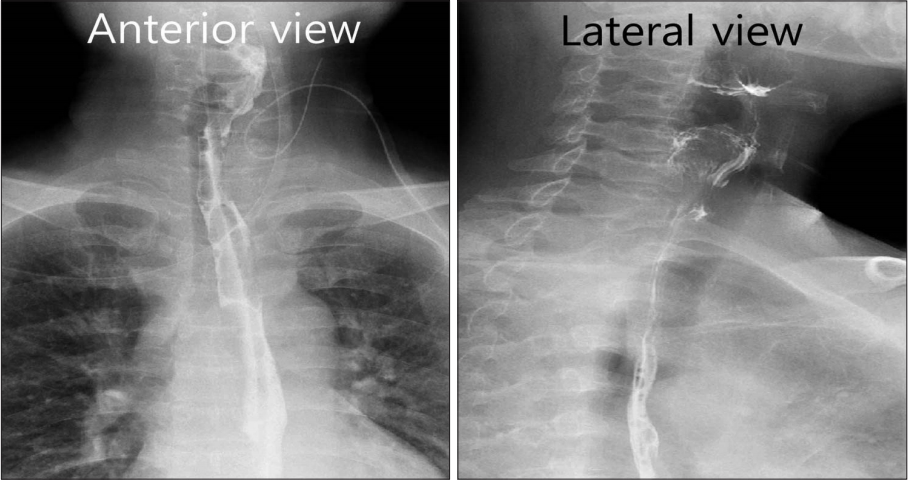
In esophagography image of after 7 days of opeartion, there are no fistula or leakage on the esophagus in both anterior and lateral view.
고 찰
1983년 Ekberg에 의해 처음 알려지게 된 KJD는 그 발병기전은 아직 명확하지 않으나 최근 그 발생이 선천적이기보다는 후천적으로, 특히 성인이 되었을 때 발생한다는 의견이 있다[3,4].
KJD는 식도조영술을 이용하여 해부학적 발생위치를 파악해서 ZD와 감별진단을 해야한다. 하지만 KJD와 ZD는 해부학적 발생위치의 차이만 있는 것은 아니다. KJD는 ZD보다 흡인과 위식도 역류와 같은 증상이 발현되는 경우가 드물며 게실의 크기도 KJD가 ZD보다 작다. 또한 KJD의 경우는 게실이 항상 좌측에 생기는데 우측에 생기는 경우는 게실이 양측으로 발생하였을 때 뿐이다. 또한 KJD의 경우 그 발생빈도가 ZD의 4분의 1로 흔하지 않아 두가지 게실은 반드시 정확한 감별진단이 필요하다[3]. 또한 본 증례의 환자는 일반적인 KJD 환자와는 다르게 경부 이물감 및 불편감과 같은 증상을 호소하였기 때문에 JD와의 감별이 더욱 중요하였고 내시경과 식도조영술 및 경부전산화단층촬영을 통해서 정확한 진단을 할 수 있었다.
1877년 Nicolandi에 의해 처음 시행된 이후로 KJD에 대한 전통적인 치료는 경부절제를 통한 접근법이었다[5]. 처음에는 사망률도 높고 위험한 술식이었으나 시간이 지나면서 수술기술이 발달함에 따라 경부절제를 통한 접근은 안전하고 효율적인 술식이 되었다. 특히 수술과정에서 가장 중요한 술식은 게실을 절제할 때 윤상인두근절제술을 시행하는 것인데 이 술식은 시간이 흐르면서 게실절제술을 시행할 때 재발을 막기 위해 반드시 시행해야 할 중요한 치료법이 되었다[6].
내시경적 접근법은 1917년 Mosher에 의해 소개된 이후로[7] 최근 20년동안 각광을 받기 시작하였는데 원래 내시경적 접근법은 종격동염의 위험성 때문에 대중성을 얻지 못했었다. 그러나 1960년에 Dohlman과 Mattsson에 의해 내시경적 게실절제술이 다시 소개되고부터 조금씩 대중성을 얻기 시작하였다[8]. ZD의 경우에는 내시경적 접근이 유용하다는 연구 결과가 있지만[9] KJD는 게실의 위치상 수술시 되돌이후두신경 손상의 가능성이 있기 때문에 경부절제를 통한 접근법이 선호된다.
본 증례의 환자는 경부의 흉터를 우려하여 내시경으로 먼저 접근을 시도하였으나 게실까지의 거리가 멀고 접근이 용이하지 않아 경부절제를 통한 수술로 방향을 선회하여 진행하였다. 게실을 절제한 이후 절제부위에 강화를 위한 목빗근회전피판술을 시행하였는데 이는 이전에 소개되었던 KJD와 관련된 여러 증례보고 및 논문에서는 시행하지 않았던 술식이다. 수술 후 일주일 째 시행하였던 식도조영술에서 수술부위의 누공 및 누출 확인되지 않아 수술이 성공적이었음을 확인할 수 있었다.
본 환자는 다른 KJD 환자와는 다르게 경부 불편감 등의 증상을 호소하였던 환자로 건강검진상 시행한 내시경에서 보인 식도게실만으로 KJD를 바로 예측하기는 어려웠다. 하지만 식도조영술을 바로 시행하여 게실이 발생한 위치로 미루어 KJD를 감별진단하였고 올바른 수술적 치료를 시행할 수 있었다. 따라서 이와 유사한 진찰 소견을 보이는 환자에서는 주기적인 외래 추적관찰과 위내시경 및 식도조영술을 통한 검사가 반드시 필요하다는 점을 염두에 두어야 하겠다.