성대 폴립으로 오인된 후두의 육종양 암종 1례
A Case of Sarcomatoid Carcinoma of the Larynx Mimicking Vocal Polyp
Article information
Trans Abstract
Sarcomatoid carcinomas are biphasic tumors which have surface epithelial changes and an underlying spindle-shaped neoplastic proliferation. A 62-year-old male with hoarseness came to our hospital for evaluation. A single smooth polypoid lesion was detected on his right true vocal fold by larnygoscope. The patient was diagnosed with vocal polyp and treated with surgical excision. Pathology report of the excised specimen was compatible with sarcomatoid carcinoma. Therefore, further surgical resection was performed to secure safety margins. We report a case of a sarcomatoid carcinoma patient who was clinically diagnosed as vocal polyp.
서 론
육종양 암종(sarcomatoid carcinoma)은 편평세포암종(squamous cell carcinoma)과 육종양 병변이 동시에 존재하는 병리학적 특징을 지니는 종양으로, 후두의 악성 종양 중 1~2%를 차지하는 드문 질환이다[1]. 국내에서는 현재까지 13예의 후두 육종양 암종이 보고되었다[2-11]. 후두 육종양 암종은 내시경상 대부분 폴립양(polypoid) 또는 유경형의(pedunculated) 양상을 보이며[1], 성대 침범시 성대 폴립처럼 보일 수 있다[4]. 육종양 암종의 경우 원발 부위의 병기가 높을 경우 예후가 나쁘며[1], 질환의 진행에 따라 급성 호흡곤란을 유발할 수 있으므로[5,10] 성대 폴립으로 오인하여 진단이 늦어지지 않도록 감별에 주의를 요한다. 저자들은 애성을 주소로 내원한 62세 남자 환자에서 성대 폴립으로 오인된 후두 육종양 암종 1예를 경험하였기에 문헌고찰과 함께 보고하고자 한다.
증 례
62세 남자 환자가 10일 전부터 갑자기 발생한 애성을 주소로 내원하였다. 환자는 30갑년의 흡연력이 있었으며 매주 소주 1병의 음주력이 있었다. 후두내시경상 우측 진성대 중반 1/3 지점에서 기원한 0.5×0.4 cm 크기의 단일 폴립 양상의 종괴가 관찰되었다(Fig. 1A). 종괴의 표면은 매끈한 양상이었으며 진성대와의 경계가 뚜렷하였다. 양측 성대의 움직임은 정상이었다. 음성 검사상 F0 144.607 Hz, Jitter 9.844%, Shimmer 23.958%, NHR(Noise-to-harmonics ratio) 0.505로 확인되었다. Stroboscopy 상 성대 점막의 진동성은 비교적 양호하였다. 우측 성대 폴립 진단하에 후두미세수술을 시행하였고, 술 중 종괴가 다소 단단한 양상이었으며, 진성대의 점막 손상을 최소화하면서 종괴를 제거하고 수술을 종료하였다. 수술 8일 뒤 후두내시경상 폴립양 종괴가 사라졌고 우측 진성대 표면이 충혈된 소견이 있었다(Fig. 1B). 술후 조직병리검사상 방추 세포의 이형성 증식이 관찰되었고 편평상피 분화의 소견은 없었으며(Fig. 2A), CK에 부분적 양성(Fig. 2B), P63에 부분적 양성으로 확인되어(Fig. 2C), 후두의 육종양 암종으로 최종 진단되었다. 이후 병기 진단을 위해 양성자 방출촬영(positron emission tomography)과 상부 위장관 내시경(esophago-gastrodudenal endoscopy)을 시행하였으며 림프절 전이나 원격 전이의 소견은 없었다. 병기는 1기(T1aN0M0)였다. 육종양 암종의 근치를 위해 후두미세수술 시행일로부터 한달 뒤 본원에서 III형 레이저 성대절제술(type III laser cordectomy)을 시행하였다. CO2 레이저를 이용하여 진성대 부분 절제를 시행하였고 육안상 충분한 안전 절제연을 확보하였다(Fig. 3). 술후 조직병리검사상 방추 세포의 이형성 증식 소견이 잔존해 있었고, 상피 내 편평상피암종(squamous cell carcinoma in situ)이 동시에 관찰되어 육종양 암종 진단을 재확인하였다. 변연 침범 소견은 없었다. 림프혈관계 침범(lymphovascular invasion) 및 신경주위 침범(perineural invasion)의 소견도 없었다. 레이저 성대절제술 10일 뒤 후두내시경상 우측 진성대의 체적이 감소하고 점막이 재생되어 수술 부위를 덮은 소견이 확인되었으며(Fig. 4), 이후 외래 통해 추적관찰 중이다.
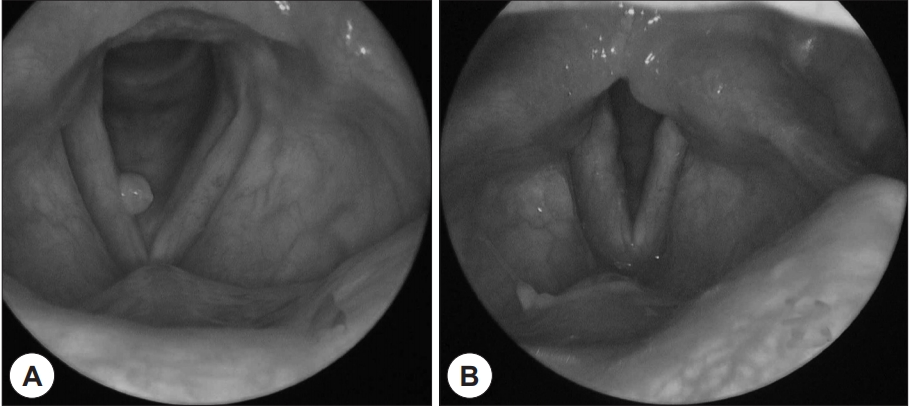
Laryngoscopic findings. A : Initial laryngoscopy showed a single smooth-surfaced polypoid lesion of right vocal fold. B : The polypoid lesion disappeared and there was hyperemia on the surface of the right vocal fold on 8 days after operation.
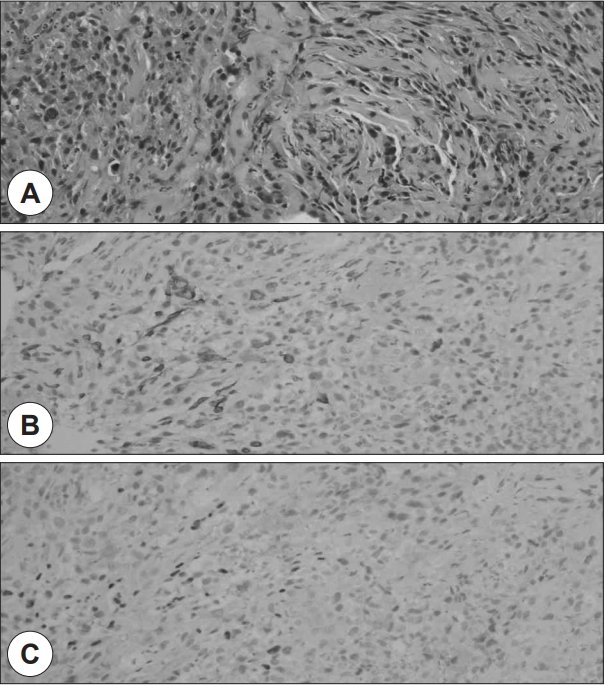
Histopathologic findings. A : Microscopic finding shows proliferation of dysplastic spindle cells and there is no definite sign of squamoid differentiation (H&E stain, ×200). B and C : Immunohistochemical finding shows focal positive staining of CK (×200) (B) and focal positive staining of P63 (×200) (C).

Intra operative microscopic finding. Type III laser cordectomy was performed.

Post-laser cordectomy laryngoscopic findngs on 10 days after operation. The volume of the operated right vocal fold was reduced and the mucosa overlying the wound was regenerated.
고 찰
육종양 암종은 후두의 악성 종양 중 1~2%를 차지하는 드문 종양이다. 남성, 60대에서 주로 발생하며, 이는 전형적인 편평세포암종과 동일하다. 흡연, 과도한 알코올 섭취와의 강한 연관성이 밝혀져 있으며, 유력한 발병 인자로 알려져 있다[1,3,12]. 방사선 치료 이후 육종양 암종이 발생했다는 보고들도 있으나[1,13], 후두 육종양 암종의 주된 원인 인자로 고려되지는 않는다[1,12]. 후두 육종양 암종의 증상으로는 1년 미만의 애성이 흔히 확인되며, 그 외 급성 호흡곤란, 연하통, 연하곤란, 인후통, 기침, 천명 등을 보일 수 있다[5].
육종양 암종은 이상성의(biphasic) 악성 종양으로, 표면에서는 상피 세포의 악성 분화를 보이고 그 심층에서는 방추 세포의 악성 분화를 보인다[1,6,12]. 병리학적으로 광학 현미경(light microscopy) 소견상 방추 세포의 악성 분화는 관찰되나 상피 세포의 악성 분화의 증거는 명확하지 않은 경우가 있으며, 이럴 경우 면역조직화학검사(immunohistochemistry)가 감별 진단에 유용하다[1,12]. 면역조직화학검사상 CK, EMA, HMWCK, p63, CK5/6, AE1/AE3에서 양성일 경우 광학 현미경 소견상 명백하지 않았던 상피 세포의 악성 분화를 확인할 수 있다[12].
Viswanathan 등의 연구에 따르면, 두경부에 발생한 육종양 암종은 구강에서 발생한 경우가 63.8%로 가장 흔하였고, 후두에서 발생한 경우는 17.5%로 2번째였다[12]. 후두에서 육종양 암종이 발생한 경우, 질환의 초기에 후두의 폐쇄로 인한 증상이 발생하여 T1 또는 T2 병기에서 조기 발견된 경우가 많았다[1,3,4].
Thompson 등의 연구에 따르면, 후두에 발생하는 육종양 암종의 98.9%가 폴립양 또는 유경형으로 점막 밖으로 자라나는 내시경적 또는 육안적 소견을 보인다[1]. 특히 성대에 발생한 육종양 암종은 성대 폴립과 임상 양상과 내시경 소견이 유사하며[2,4,6], 따라서 임상 양상이나 내시경 소견만으로는 진단이 어렵다[6]. 실제로 국내에서도 성대 폴립으로 오인된 사례가 3예 보고되었고[2,10,11], 그 중 1예에서는 후두미세수술 시행 18일 후 발생한 호흡곤란으로 응급기관절개술을 필요로 하였다[10]. Hong 등의 증례에 따르면, 후두 내시경상 성대의 폴립양 양성 종양으로 생각되었던 육종양 암종에서 성대 폴립 절제술 시행시 본 증례처럼 병변이 일반적인 폴립보다 단단한 양상이 확인된 바 있어[6], 감별 진단시 고려할 점으로 사료된다.
치료는 전형적인 편평세포암종에 준하여 시행하는 경우가 많다[14]. 그러나 육종양암종은 전형적인 편평세포암종보다 더 침습적이고 재발을 잘 하는 특성이 있어, 조기 병변에서 방사선 치료만 시행할 경우 재발율이 높다는 견해가 있다[4,15].
본 증례에서 진성대에서 기원한 단일 폴립 양상의 종괴가 관찰되었고, 종괴의 크기가 작고 표면이 매끈하며 진성대와의 경계가 뚜렷하여 성대 폴립으로 판단하고 후두미세수술을 시행하였다. 그러나 조직병리검사상 육종양 암종으로 진단되어 레이저 성대절제술을 추가로 시행하였다. 국내에서 후두의 거대한 단일 폴립 양상의 병변에서 육종양 암종이 발견된 다른 증례 보고가 있었으나[4], 0.5×0.4 cm 수준으로 크기가 작은 단일 폴립 양상의 종괴에서 육종양 암종이 진단된 것은 최초의 사례이다. 흡연, 음주의 과거력이 있는 환자에서 성대의 종괴가 발생시 단일 폴립양 종괴로 크기가 작고 표면이 매끈하며 경계가 명확하더라도 육종양 암종 등의 드문 후두 악성 종양의 가능성을 완전히 배제해서는 안 될 것으로 사료된다.