하인두 내에 발생한 유경성 섬유지방종 1예
Pedunculated Fibrolipoma of the Hypopharynx: A Case Report
Article information

Trans Abstract
Fibrolipomas are a rare microscopic variant of lipomas, characterized by mature adipose tissue interspersed with dense fibrous connective tissue. These lesions are rarely observed in the head and neck region and represent <0.6% of all benign tumors of the larynx and hypopharynx. Their clinical presentation depends on the location and size of lesions. Patients present with variable symptoms; however, fibrolipomas of the larynx and hypopharynx are clinically important because these tumors can cause unpredictable airway obstruction, particularly during general anesthesia induction. We present a case of a hypopharyngeal fibrolipoma in a 61-year-old patient with frequent dyspnea, dysphagia, and muffled voice. Laryngoscopy revealed a well-demarcated pedunculated ovoid mass involving the larynx. We performed laryngomicrosurgery using a carbon dioxide laser for surgical excision and subsequent evaluation confirmed the diagnosis of fibrolipoma. We report a case of hypopharyngeal fibrolipoma, together with a literature review.
서 론
지방종(lipoma)은 피하 지방 조직에서 발생하는 양성 종양으로 두경부 영역에서는 주로 후경부에 발생하며, 피부 아래에서 잘 움직이고 부드러운 양상의 혹이 만져지면 의심해 볼 수 있다[1]. 하지만 하인두 내에 지방종이 발생하는 경우는 굉장히 드물고, 하인두에 발생하는 양성 종양 중에 지방종의 비율은 1% 미만으로 알려져 있다. 흔히 발생하는 종양은 아니지만 크기가 큰 경우 드물게 기도를 막아 호흡 곤란을 일으키기도 한다[2].
최근 저자들은 위내시경 검사에서 발견된 작은 하인두 종양이 4개월 만에 갑작스럽게 크기가 증가하여 호흡 곤란, 연하 장애를 호소한 환자에게 CO2 레이저 수술을 통해 종양을 제거하고, 섬유지방종(fibrolipoma)으로 최종 진단된 1예를 경험하였기에 문헌고찰과 함께 보고하고자 한다.
증 례
폐결핵을 앓은 기왕력과 고혈압이 있는 61세 남자 환자가 1달 전부터 음식을 먹을 때 목에 걸리는 느낌과 운동 시에 숨이 차는 증상을 주소로 본원에 내원하였다. 최근 코골이가 심해졌고, 1달 동안 8 kg의 체중 감소가 있었다. 환자는 타병원에서 내원 5개월전 시행한 위내시경 검사상 우연히 하인두 부위에 종양이 발견되었으나, 특별한 증상이 없고 크기가 작아서 지켜보자는 말을 들었다. 본원에 내원하여 후두 내시경 검사를 시행하였고, 우측 하인두 측벽에 경(stalk)을 가진 난원형의 종양이 상기도를 막고 있는 소견이 관찰되었다(Fig. 1A). 호흡 및 기침 시 종양이 위아래로 움직이는 소견이 보였고 성대 움직임은 이상이 없었다. 경부전산화단층촬영검사(neck CT)상 하인두의 측벽에서 유래한 약 3 cm 크기의, 조영 증강이 되지 않으며 지방 조직과 동일한 감쇠(attenuation)를 보이는 점막 하 종양이 관찰되었다(Fig. 1B and C). 증상 조절을 위해 수술적 제거를 계획하였고, 수술 시 마취과 전문의가 비디오경성삽관용후두경을 이용하여 종양을 젖히면서 문제없이 기도 삽관을 시행하였다. 현수 후두경을 삽입한 후 수술현미경 시야에서 미세 겸자로 종양의 경이 있는 부위를 잡고 견인한 후 CO2 레이저(3 watt, super pulse mode)를 이용하여 종양을 절제하였다. 경의 절제연에서 동결 절편 검사를 시행하였고, 악성 소견은 없음을 확인하고 수술을 종료하였다. 절제된 종양은 매끈한 점막을 가진 난원형 종양으로 크기는 3.5×3×2 cm이었다(Fig. 2A). 조직병리학적 검사에서 종양은 성숙한 단일 공포성의 지방세포로 구성되어 있었고, 간질성 콜라겐성의 섬유화 소견이 관찰되어 최종적으로 섬유지방종으로 진단되었다(Fig. 2B and C). 환자는 특별한 문제없이 수술 후 1일째 퇴원하였고 2년 6개월이 지난 현재까지 특이소견 없이 외래 경과관찰 중이다(Fig. 2D).
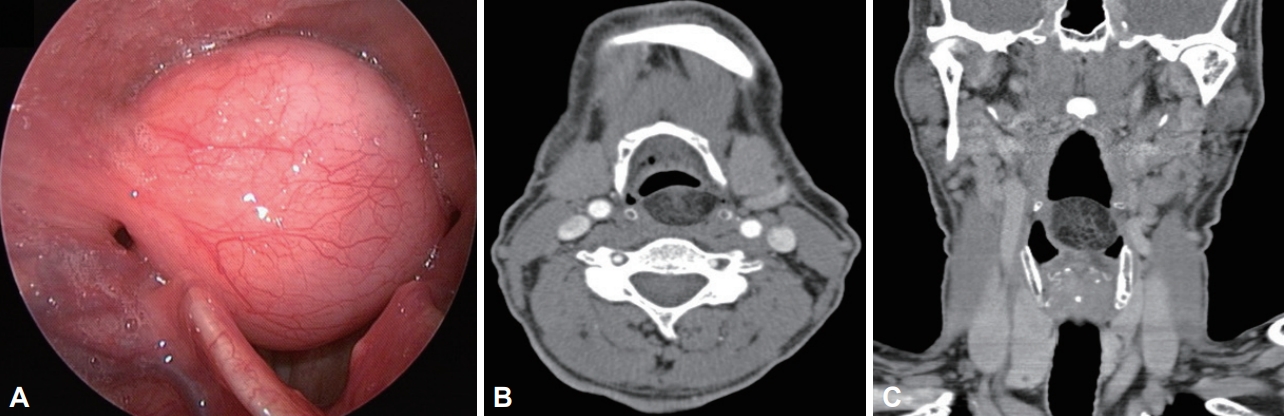
Laryngoscopic finding shows a large pedunculated mass arising from the right lateral wall of hypopharynx (A). Preoperative contrast-enhanced computed tomographic images. Axial (B) and coronal (C) CT scans show the pedunculated submucosal fatty mass of hypopharynx.
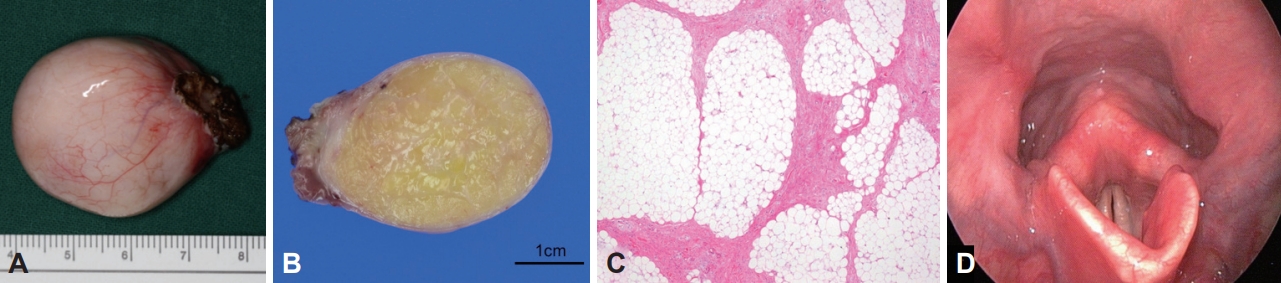
The surgical specimen is ovoid and smooth surfaced, measuring 3.5×3×2 cm (A). Grossly, the mass is pedunculated and its cut surface is pale yellow on cut section (B). On microscopic examination, the tumor is composed of mature and univacuolated fat cells with interstitial thick collagenous fibrosis (C) (H&E stain, ×100). Recent postoperative photographs show normal looking finding without any suspicious pathologic finding of the hypopharynx (D).
고 찰
외래로 내원한 환자가 호흡 곤란, 연하 장애, 천명, 경부 이물감 등을 호소한다면 후두 내시경 검사를 통해 인후두 영역의 이상을 확인해야 한다. 상기 증상이 빠르게 진행되는 양상일 경우에는 종양이 있는지를 확인하고 악성 여부를 감별해야 한다. 간혹 하인두와 연결된 부위인 경부 식도(cervical esophagus)에서 유래된 종양이 크기가 커져서 인후두 부위로 역류(regurgitation)하여 증상을 일으킬 수도 있다[3]. 환자가 증상이 없더라도 위내시경 검사를 하다가 우연히 후두덮개낭종(epiglottic cyst)이나 지방종이 발견되는 경우가 있는데 검사를 시행한 전문의가 수술이 필요한지 여부를 판단해야 한다[4].
하인두에 생기는 지방종은 발생 빈도는 낮지만 발성이나 호흡 그리고 저작활동을 방해할 수 있을 정도로 크게 자라는 경우도 있다[5]. 이런 경우 호흡 곤란이나 삼킴 곤란, 목의 이물감을 느낄 수 있으며 수면무호흡증이나 코골이도 나타날 수 있다[6]. 상기도를 막을 정도로 크기가 커지면 기도 폐쇄가 생기는 경우도 드물게 있고 증상은 갑작스럽게 악화될 수 있다[7]. 종양이 상기도를 막을 정도로 큰 경우에는 전신마취를 위한 기관 삽관이 쉽지 않고 경부접근법을 통한 수술이 필요한 경우도 있기 때문에 수술 전에 영상학적 검사가 필요하다. CT에서는 지방종의 경우 균질하고 낮은 감쇠 병변을 보이는 것이 특징이며[8], MRI에서는 피하지방층과 동일한 신호 강도를 보이며, 조영 증강이 되지 않는 것이 특징이다[9].
지방종은 다양한 조직병리학적 특성을 가지며, 세부 분류로는 섬유지방종, 점액지방종(myxofibroma), 연골 지방종(chondroid lipoma), 방추세포 지방종(spindle cell lipoma), 다형성 지방종(pleomorphic lipoma) 그리고 혈관지방종(angiolipoma) 등으로 나눌 수 있다[10]. 그 중 섬유지방종은 지방종의 드문 조직학적 아형 중 하나로, 성숙한 지방 조직이 치밀한 섬유성 결체조직 내로 파고들어와서 생기는 것을 특징으로 한다[11].
수술적 절제는 지방종의 최우선 치료 방법이다. 이전의 보고들에 의하면 후두 근처에 발생한 지방종은 재발이 가능하며 드물게 악성화 되는 경우도 있다. Laurent 등[12]은 하인두에 발생한 재발성 지방종이 악성 섬유성 조직구종(malignant fibrous histiocytoma)으로의 악성화가 진행된 환자에서 가측 인두절개 접근법(lateral pharyngotomy approach)을 통한 종양 절제를 시행한 후 2년간 재발 없음을 보고하였으며, Reibel과 Greene[13]은 흉부 및 경부의 외부 절개를 통해 9×6×3 cm 크기의 식도 섬유지방종을 절제한 후 9년 뒤에 후 인두에서 지방육종이 발생한 환자에서 광범위 절제술 및 술 후 방사선 치료 후 13개월 간 재발없이 추적 관찰한 증례를 보고한 바 있다. Sotirovi´c 등[14]은 하인두 지방종이 재발하여 내시경적 절제술을 3차례 시행한 후에 4.6×3.2 cm 크기의 지방육종이 발병한 환자에서 가측 인두절개 접근법을 통한 종양 절제 후 5년 동안 재발없이 추적 관찰한 증례를 보고하였다. 상기 증례들을 고려하면 하인두의 지방종은 드물지만 재발이 잦은 경우 악성화의 가능성이 있기 때문에, 술 전에 종양의 크기와 위치를 파악하여 적절한 수술 접근 방법을 통해 종양을 완전히 절제하는 것이 도움이 될 것으로 생각된다[15]. 경구강 수술은 수술 후 회복이 빠르고 합병증이 적은 것이 장점이나 완전 절제가 쉽지 않은 경우에는 경부 접근법을 고려해야 하며, 종양의 크기로 인해 기관 삽관이 어려울 때는 수술 전 기관 절개술이 필요한 경우도 있다.
위 내시경에서 하인두 부위에서 우연히 발견된 작은 종양은 육안적으로 악성이 의심되지 않는다면 일반적으로 적극적인 치료를 하지 않는다. 하지만, 일부 보고들에서 알 수 있듯이 인후두 영역에 생기는 지방종의 경우 크기가 커지면서 여러 증상들을 유발할 수 있으며, 수술적 치료 후에도 재발하는 경우들이 있다. 하인두 영역에서 우연히 발견된 종양에 대하여 크기, 위치 및 병변의 양상을 고려하여 증상 진행 가능성 및 악성화 가능성을 확인하고, 필요 시 영상학적 검사를 시행하여 수술적 처치의 필요성을 평가해야 한다. 증상이 없거나 크기가 작더라도 환자에게 적절한 설명을 제공하고, 추적 관찰을 통해 종양의 변화 양상을 확인하며, 필요 시에는 조직검사 또는 수술적 제거를 적극적으로 고려하는 것이 환자의 예후에 도움이 될 것으로 생각한다.
Acknowledgements
None.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Authors’ Contribution
Conceptualization: Tae Seong Eo, Ji-Hoon Kim. Data curation: Tae Seong Eo, Hyang Ae Shin, Jeong Hae Kie. Formal analysis: Tae Seong Eo, Hyang Ae Shin, Jeong Hae Kie. Methodology: Tae Seong Eo, Ji-Hoon Kim. Visualization: Tae Seong Eo, Jeong Hae Kie. Writing—original draft: Tae Seong Eo, Ji-Hoon Kim. Writing—review & editing: Tae Seong Eo, Ji-Hoon Kim. Approval of final manuscript: all authors.