후두로 돌출된 설인신경 신경초종 1예: 증례보고
A Case of Glossopharyngeal Schwannoma Protruding to the Larynx: A Case Report
Article information

Trans Abstract
Schwannoma is benign tumor that can occur in any part of the nerve that contains a Schwann cell. It is rare in the head and neck region and is characterized by common postoperative neurologic symptoms. We experienced a cervical schwannoma in a 22-year-old young man. Except for a foreign body sensation in the neck and a mass in the anterior region, there were no other complaints. A retropharyngeal schwannoma was most suspected considering neck computed tomography, magnetic resonance imaging, laryngoscopy and fine needle aspiration. Surgical treatment was performed, and the origin of the schwannoma was diagnosed as the tonsillar branch of the glossopharyngeal nerve. Histopathological examination confirmed the presence of a schwannoma with typical characteristics. After surgery, the patient recovered without any side effects. We report this case with a review of the literature.
서 론
신경초종은 신경초세포(Schwann cell)로 쌓여있는 신경에서는 어디서든 발생할 수 있는 양성종양으로 1910년 처음 소개되었다[1]. 전체 신경초종의 25%-45%가 두경부 영역에서 발견되며 두경부 내에서 전경부에서 발생한 신경초종은 아주 드물다[2]. 한 후향적 연구결과에 따르면 경부 영역의 많은 신경 중에서 국내에서는 미주신경과 교감신경 기원 신경초종 기원이 가장 흔하였으며[3,4], 대부분의 경우 수술 후 성대마비, 호너 신드롬 등의 신경학적 증상을 합병증으로 보고하고 있다[5-7]. 수술 전 종양의 위치와 원발부위를 찾기 위해 영상학적 평가가 이루어지고 기원신경을 추정하게 된다[8]. 저자들은 전경부 종괴로 내원한 22세 남자 환자에서 후인두강 기원 신경초종으로 의심되었으나 설인신경(glossopharyngeal nerve) 기원의 신경초종을 적출하였고, 수술 후 어떠한 부작용도 없이 치료한 드문 증례를 경험하여 문헌고찰과 함께 보고하는 바이다.
증 례
평소 건강하던 22세 남자 환자가 2년전부터 발생한 목 이물감, 우측 전경부 종물을 주소로 내원하였다. 해당 종물에 대해 타병원에서 전산화단층촬영 및 자기공명영상검사를 진행하여 신경초종에 준하는 소견을 보였고 초음파 유도하 세침흡인세포검사(fine needle aspiration)를 시행한 결과 신경초종이 진단되어 미주신경 기원이 의심된다는 소견을 받고 수술적 치료를 원하여 본원으로 입원하였다. 후두내시경상에서 하인두 부위에 종양으로 인해 돌출된 부분이 관찰되었으며(Fig. 1), 경부전산화단층촬영에서 후인두공간 외에 주위 와 경계가 명확한 4.6×4.4 cm의 원형의 종물이 관찰되었고 종양의 변연부의 반점 양상의 조영증강된 부분이 관찰되었다(Fig. 2A) 자기공명영상검사상 T1 강조영상에서 저신호 강도의 종물이 경동맥과 경정맥을 후외측으로 전위시키는 소견을 보였고(Fig. 2B) 조영증강 T1 강조영상에서는 과녁징후(target sign), 낭성변화가 두드러져 보였으며(Fig. 2C), T2 강조영상에서는 소금후추가루양상(salt and pepper appearance)이 관찰되었다(Fig. 2D). 연부조직의 경계가 잘 구별 지어지는 자기공명영상에서도 후인두공간과 종양의 관계가 명확하지 않았다. 영상학적 평가를 고려하였을 때 상기 종물은 미주신경 기원보다는 후인두공간 기원 혹은 교감신경절 기원 신경초종으로 추정되었다. 이에 대해서 수술 후 발생할 수 있는 호너신드롬이나 삼킴장애 등의 가능성에 대해서 설명하였으나, 합병증 발생 가능성에도 불구하고 환자가 수술을 적극적으로 선호하여 이에 대해서 동의를 받은 후에 경부로 접근하여 수술적 제거를 계획하였다.
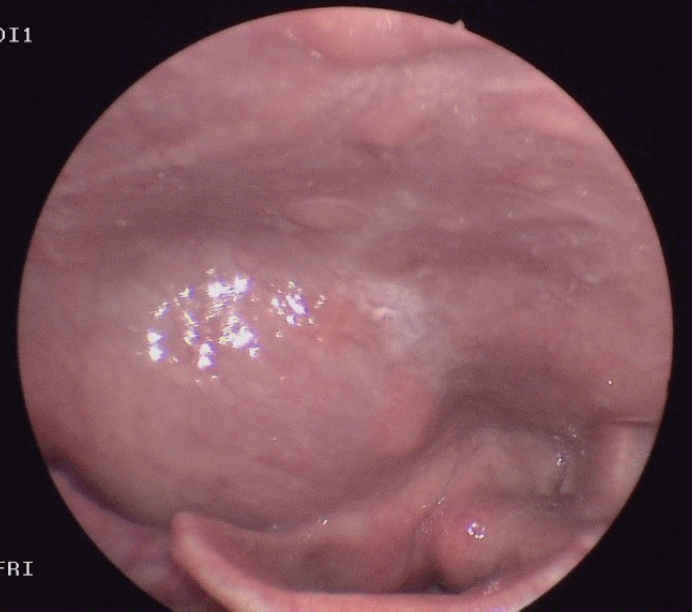
Endoscopic photographs of the patient’s pharyngeal wall. The margin of the mass protruding into the posterior wall of the hypopharynx is observed on laryngoscopy.
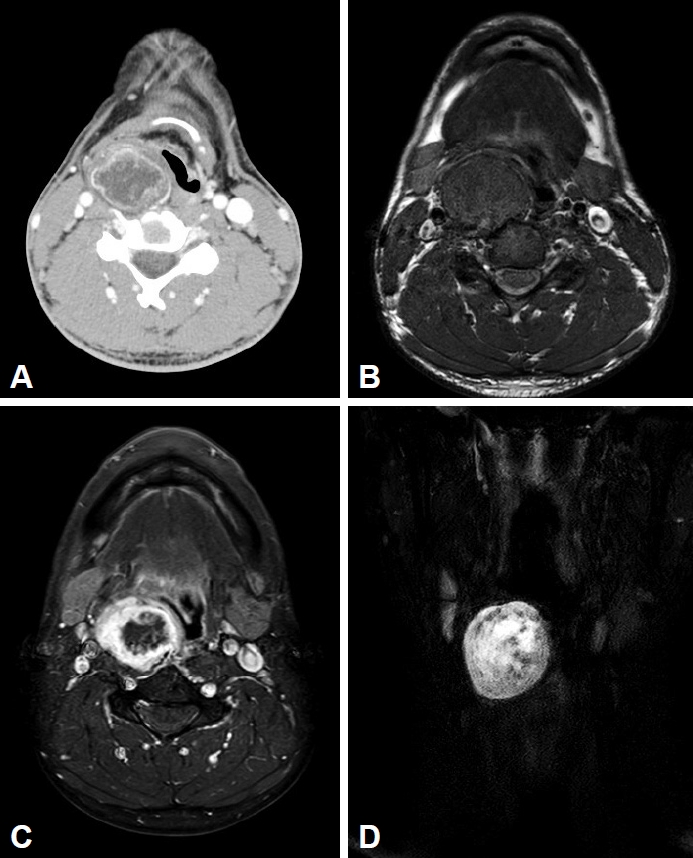
Axial and Coronal view of Neck CT and MRI scan. A: Round shape mass with margin enhancement. B: T1-weighted axial MRI image shows low round shape mass signal density. C: T1-weighted gadolinium MRI image shows significant target sign and cystic change. D: T2-weighted coronal MRI image shows intense enhancement with salt and pepper appearance.
수술은 설골 높이에서 외측 피부 주름을 따라 4 cm 피부 절개 후 위아래로 광경근하 피판을 들고 흉쇄유돌근을 외측으로 견인, 피대근을 박리하여 경부 내장공간(visceral space)이 노출되게 하였다. 해당 부위에서 종물을 쉽게 확인할 수 있었으며 피막에 쌓여져 주위와의 경계가 분명한 특징을 가지고 있었다. 기원 신경은 종물의 크기로 인해 확인이 어려워 피막절개를 시행한 뒤 손가락을 이용한 무딘 박리(blunt dissection)로 종양의 보존적적출(enucleation)을 완료하였다. 적출 후 기원 신경이 경동맥공간보다 전내측에서 주행하는 것이 관찰되었고(Fig. 3A) 미주신경은 경동맥과 경정맥 사이로 주행하는 것이 확인되어 미주신경 기원의 가능성을 배제하였다. 신경의 굵기와 주행경로를 보았을 때 설인신경의 편도분지(tonsillar branch)로 추정되었다. 그 외 다른 조직과의 유착이나 연결은 없었고 배액관을 유치한 후 수술을 종료하였다. 육안적 소견상 종양은 잘 피막화된 견고한 종물의 형태였으며 크기는 4.5×4.0×3.0 cm로 단면은 노란 표면에 오래된 출혈과 부분적 점액질 소견이 관찰되었다(Fig. 3B and C). 조직 검사상 hematoxylin and eosin (H&E) 책상 배열(palisading pattern)을 이루는 방추형의 신경초세포 핵이 관찰되었으며, 세포가 밀집되어 베로카이 소체(verocay body)를 형성하고 출혈의 흔적으로 인한 혈전 형성이 확인되었다(Fig. 4). 술 후 환자는 특별한 불편감을 느끼지 않았으며 수술 후 시행한 후두경 상에서 종물이 깨끗하게 제거된 상태가 확인되었다(Fig. 5). 또한, 삼킴이나 미각의 장애, 성대마비 등의 합병증 없이 수술 후 4일째 퇴원하였고, 이후 정기적인 추적관찰 중에도 특별한 문제없이 지내고 있다.

Intraoperative photographs. A: Originating nerve (asterisk) of schwannoma is observed running over the common carotid artery after enucleation. B: Surgical specimen. C: Traces of hemorrhage with cystic change was observed on cross-section of the specimen.

Histopathologic findings of glossopharyngeal schwannoma. A: Verocay body with biphasic feature with compact areas of spindle cells (Antoni A area) and loosely arranged hypocellular foci (Antoni B area) (H&E, ×100). B: Thrombus formation around the small vessel (H&E, ×400).
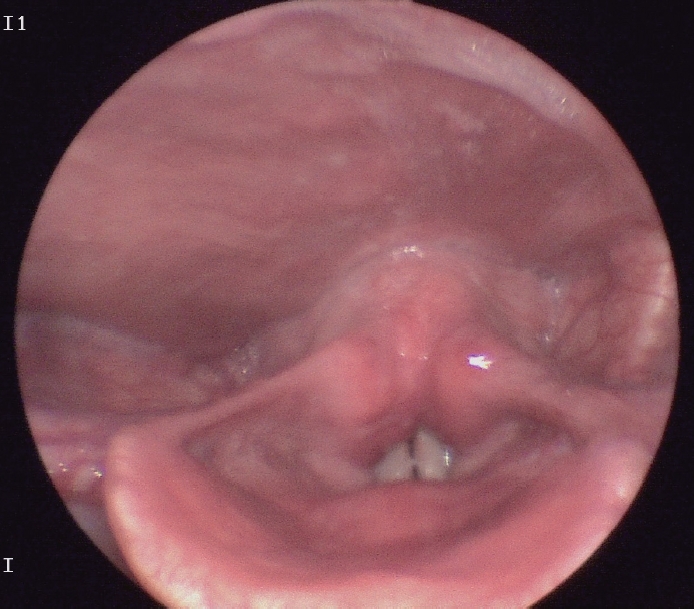
Postoperative endoscopic photographs of the patient’s pharyngeal wall. The protruding lesion in the wall of the pharynx was removed.
고 찰
신경초종은 신경초세포가 이루는 신경초로 덮여있는 신경에서는 어디에서나 발생할 수 있는 양성종양으로 Verocay[1]에 의해 “Neurofibrome”으로 정의되었으며 서서히 성장하고 단발적 발생을 특징적으로 하고 피막에 의해 잘 쌓여져 주변과 경계가 명확한 형태를 보인다. 전체 신경초종 중 25%-45%가 두경부 영역에서 발생하며 부인두강과 경부 level에서는 level II가 가장 흔한 호발지역으로 분류된 바 있다[2,3]. 국내의 연구에서는 미주신경과 교감신경절이 가장 대표적인 발생 부위로 알려져 있다[3]. 경부종물을 가장 흔하게 호소하고 30, 40대에 흔한 것으로 알려져 있으며 성비에서의 차이는 없다고 보고된다[4,5]. 신경초종은 전산화단층촬영에서는 근육과 비슷한 저밀도 음영을 보이며, 자기공명영상검사상 T1 강조영상에서는 저신호강도를 보이고, T2 강조영상에서는 고신호강도를 보인다. 다양한 정도의 조영증강을 나타내며 종양에서 신경의 진입 또는 진출 징후(nerve entering or existing sign), 지방 분할 징후(split fat sign), 과녁 징후, 낭성변화 등이 대표적인 소견들이다[8].
본 증례에서는 20대 남성의 신경초종으로 호발연령과 거리가 있었으며, 부인두강이 아닌 비교적 드문 호발부위인 경부 level III의 내장공간에서 신경초종이 기원하였다. 또한 수술 직후 및 경과관찰 기간에도 어떠한 신경학적 합병증이 발생하지 않았다. 자기공명영상검사에서는 과녁징후와 낭성변화가 뚜렷이 관찰되어 신경초종의 전형적 소견을 보였다.
경부는 여러 신경이 주행하여 영상검사만으로 수술 전 신경초종의 기원 신경을 특정짓는 것은 어렵기 때문에 영상학적 평가 및 수술을 통한 육안적 확인이 중요하다. 전산화단층촬영과 자기공명영상이 주로 수술 전 평가에 이용되며 주위 조직으로의 침범 및 크기를 정확히 측정하고 위치를 특정하는데 도움을 준다. 가장 흔한 호발부위 중 하나인 경부 교감신경절은 경동맥공간의 내측 후방으로 주행하기 때문에 교감신경절 신경초종은 해부학적 구조상 많은 경우에서 경동맥 공간을 전외측으로 이동시키며, 미주신경 기원 신경초종은 경동맥과 경정맥을 분리시킨다는 특징이 있다[9]. 본 증례에서는 내시경 상에서 종물로 인한 하인두 벽으로의 돌출이 관찰되고 경동맥공간의 후외측으로의 이동양상을 고려했을 때 후인두 공간 기원이 더 강하게 의심되었다. 그러나 후인두공간은 대부분 지방과 임파선 조직으로 채워져 있고 미주신경과 설인신경, 교감신경총의 작은 분지들이 인두신경총(pharyngeal plexus)을 이루며 후인두공간의 경계에 분포하기 때문에 기원신경을 정확히 특정하여 관찰하기 힘들다[10]. 그러나 본 증례에서는 기원 신경이 수술 중에 육안으로 경동맥 공간 전내측으로 수직으로 주행하는 모습이 정확히 관찰되었고, 수술 후 환자가 느끼는 불편감이 전혀 없었으며 다른 부작용 또한 발생하지 않았다. 경부의 해부학적 구조를 고려하였을 때 설인신경의 인두분지(pharyngeal branch) 혹은 편도분지가 원발부위로 가장 의심되었다.
설인신경은 두개내 및 경부의 신경초종을 모두 유발할 수 있다. 경정맥공을 통해서 미주신경, 부신경(accessory nerve)과 같이 경부로 뻗어나오기 때문에 신경초종의 위치에 따라서 덩이효과(mass effect)로 인한 압박으로 어깨 근육의 움직임이나 발성, 삼킴장애, 구역반사 조절에 장애를 일으킬 수 있다. 본 증례에서 상기 증상들에 대해서 충분히 이학적 검사를 시행하였고, 경정맥공과 거리가 있고 경동맥의 분지보다도 아래에 종양이 위치해 있어 다행히도 미주신경과 부신경의 압박으로 인한 증상들은 동반되지 않았다[11]. 설인신경은 6가지의 분지로 나뉘게 되는데 그 중 경동맥 공간 내측으로 주행하는 분지는 인두분지와 편도분지가 있다. 인두분지는 여러 연구들을 통해 미주신경과 더불어 삼킴반사(swallowing reflex)에 큰 영향을 준다고 알려져 있으며, 편도분지는 편도의 감각 및 경구개감각을 담당한다고 보고된다[12]. 따라서 이번 증례에서는 종물이 내장공간의로의 확장으로 설골까지 도달한 점, 미주신경이 정상으로 명확히 확인된 점, 수술 후 환자의 불편감 및 삼킴장애를 포함한 어떠한 부작용이 전혀 나타나지 않았다는 점에서 설인신경의 편도분지를 원발부위로 진단할 수 있었다.
병리 조직학적으로 신경초종은 두가지의 구분되는 세포 영역을 갖는다. Antoni A 영역은 세포가 밀집되어 있으며, 핵이 일렬로 늘어서 있는 베로카이 소체라는 특징적인 소견을 보인다. Antoni B 영역은 세포가 적으며 세포들의 배열이 불규칙하다. 이 영역들의 비율은 종양마다 차이가 있는데 본 증례에서는 Antoni A 영역과 Antoni B 영역이 명확히 구분되고 핵이 일렬로 늘어선 책상배열 및 베로카이 소체도 잘 관찰되며 출혈의 흔적으로 보이는 혈전의 형성이 뚜렷이 나타나 낭성 변성(cystic degeneration)을 동반한 신경초종으로 진단되었다[13].
신경초종의 주된 치료는 경부 절개를 통한 수술적 완전 절제이며, 드물게 악성화의 가능성이 있어 면밀한 추적관찰이 필요하다[14]. 저자들은 신경의 보존을 위해 보존적 종양적출술을 시행하였으며, 재발 및 잔존 조직의 악성화의 가능성을 고려하여 외래를 통해 지속적인 추적 관찰을 시행 중이다.
Acknowledgements
None
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Authors’ Contribution
Conceptualization: Su Il Kim. Data curation: Je Ho Bang, Seung Yup Son. Formal analysis: Je Ho Bang, Jong Hwan Lee. Methodology: Su Il Kim. Project administration: Je Ho Bang, Seung Yup Son. Supervision: Su Il Kim. Writing—original draft: Je Ho Bang. Writing—review & editing: Su Il Kim, Je Ho Bang. Approval of final manuscript: all authors.