선천성 후두개곡 낭종을 동반한 후두연하증의 성문상부교정술 2예
Two Cases of Laryngomalacia With Congenital Vallecular Cyst Treated by Supraglottoplasty
Article information

Trans Abstract
Vallecular cyst consisted of a unilocular cystic mass of variable size arising from the lingual surface of the epiglottis and containing clear fluid is a rare occurrence in children. Although a cyst is benign, it may cause serious airway obstruction and even death if not treated appropriately. Also, laryngomalacia is the most common congenital anomaly that causes inspiratory stridor and airway obstruction in the newborn. Symptoms typically begin to appear at around 2 to 3 weeks of age and become worse between 4 and 8 months. With a review of literature, we report two cases of vallecular cyst with symptomatic laryngomalacia in a 1-month-old female and a 2-month-old male. Both patients experienced symptom relief after undergoing endoscopic supraglottoplasty.
서 론
후두개곡 낭종(vallecular cyst)은 양성 낭종이지만 호흡곤란, 수유곤란, 흡기성 천명 등과 같은 증상들을 유발할 수 있으며, 적절한 시기에 치료를 하지 않으면 갑자기 기도 폐쇄로 인해 호흡곤란이 발생할 수 있고 심하면 사망에 이를 수 있다[1,2].
또한, 후두연화증(laryngomalacia)은 주로 영아에서 발생하며, 후두개곡 낭종과 마찬가지로 호흡곤란, 섭식장애를 일으킨다[3]. 후두연화증은 대부분 경과관찰하면 자연 호전되지만 호흡곤란이나 섭식장애가 심한 경우에는 수술적 치료가 필요하다. 후두개곡 낭종은 내시경적 수술로 종양을 제거함으로써 치료할 수 있으며, 후두연화증 역시 내시경을 이용하여 성문상부교정술(supraglottoplasty)을 시행하여 치료할 수 있다[2-4].
본 증례에서는 호흡 및 연하곤란을 주소로 내원한 소아 2예에서 후두개곡 낭종과 동반된 후두연화증을 진단하고 치료하였기에 문헌고찰과 함께 보고하고자 한다.
증 례
증례 1
재태주수 37주 1일, 2.1 kg의 여아는 생후 3주경부터 흉골 상부 함몰(suprasternal retraction) 소견과 함께 그렁거리는 숨소리가 관찰되었다. 그 후 반복되는 흡인 소견과 호흡곤란이 발생하여 소아과로 내원하였다. 후두연화증, 연하 장애 및 역류성 식도염 의증 하에 시행한 기관지내시경 검사상, 후두개 앞쪽에 위치한 후두개곡 낭종 및 후두연화증 소견이 보여 이비인후과로 협진의뢰었다. 후두개곡 낭종으로 인해 수유 곤란 및 천명(stridor)이 발생하였을 것으로 생각되었고, 후두경하 수술을 시행하기로 하였다. 전신 마취 과정에서 거대한 후두개곡 낭종으로 인해 기관 삽관이 실패하여, 고유량 비강 산소 공급 장치(high-flow nasal oxygenatiuon)를 통해 산소를 공급하며 후두경하 낭종 조대술을 먼저 시행하여 기도를 확보한 뒤 기관 삽관을 시행하였다. 낭종 제거 후 시행한 내시경 검진 상, 짧은 피열연골후두개 주름과 후방 전위된 후두개 및 후두 주변의 과잉 조직들이 관찰되는 후두연화증이 관찰되었다. 상기 소견에 대해 성문상부교정술 및 흡수성 봉합사(PDS 3-0)를 이용하여 후두개 고정술을 함께 시행하였다(Fig. 1). 수술 3일 뒤 기관 삽관을 제거하고 산소 포화도가 95% 전후로 유지가 되었으나, 지속되는 흉골하부 함몰(subcostal retraction) 및 천명에 대해 다시 한번 후두경하 상기도의 재평가를 시행하였고, 후두 상하방에서 관찰되는 약간의 삼출물을 제거하는 2차 수술을 시행하였다. 또한, 지속되는 역류성 식도염 및 연하곤란으로 위적추벽성형술(fundoplication) 및 위조루술(gastrostomy)을 시행하였다. 수술 이후 호흡곤란의 소견은 관찰되지 않았으며 식이량의 적절한 증가로 퇴원하였다. 수술 후 8개월 동안 호흡곤란 없이 경구 식이 원활하며, 재발의 소견없이 경과 관찰 중이다.
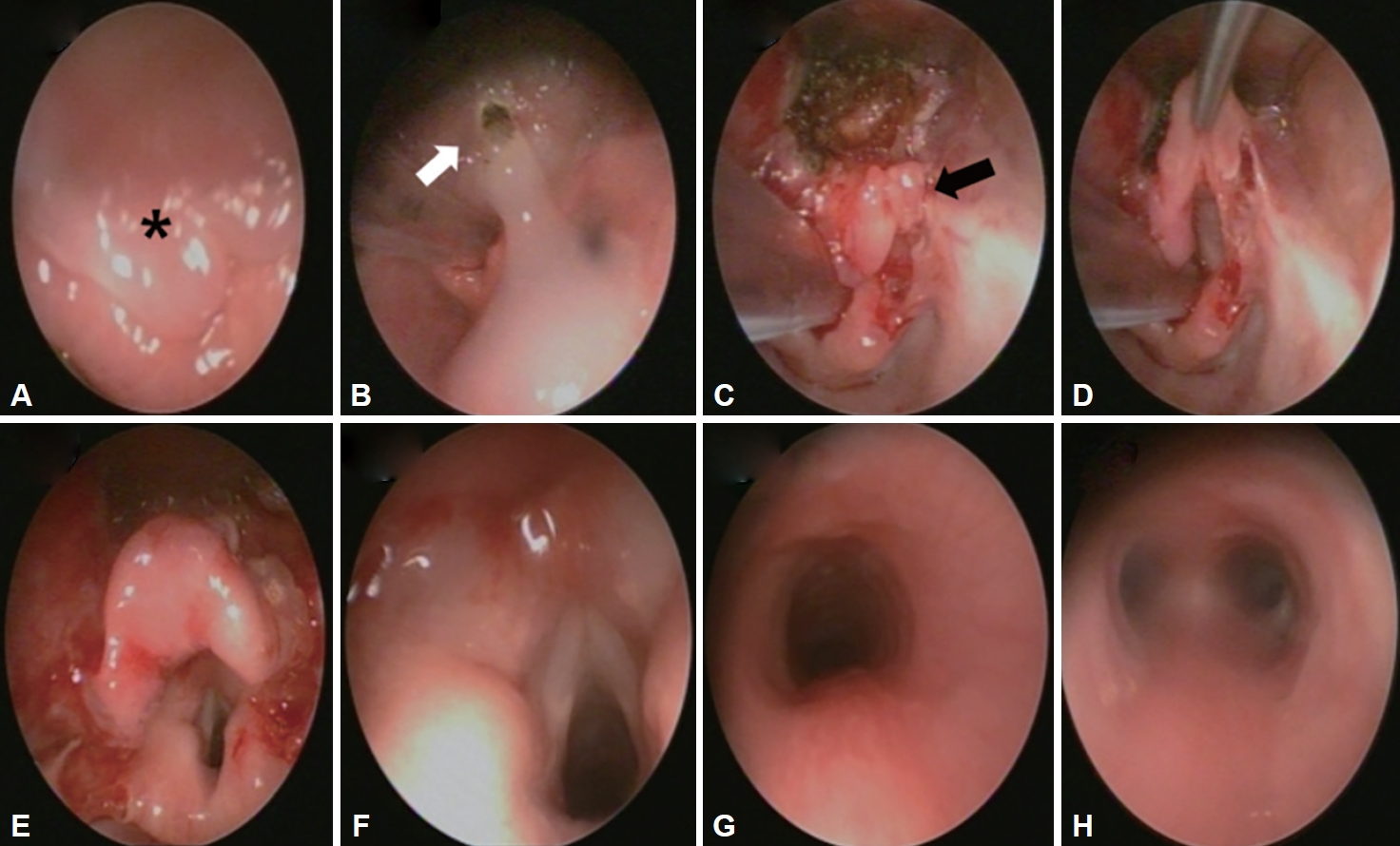
Case 1. Vallecular cyst excision and supraglottoplasty. A: No visible larynx due to large vallecular cyst and laryngomalacia (black asterisk). B: Visible lower airway after vallecular cyst expiration (white arrow). C: After vallecular cyst removal, shortened aryepoglottic fold and retroflexed epiglottis (black arrow) was identified. D: Simulation of supraglottoplasty. E: Supraglottoplasty-epiglottopexy by PDS 3-0. F: Well visible airway after supraglottoplasty. G: normal cricoid cartilage and cervical trachea. H: normal carina and bronchus.
증례 2
재태주수 39주, 3.5 kg 자연분만으로 태어난 남아는 출생 후 경구 수유시 마다 흡인이 의심되는 소견이 보이고, 호흡시 천명이 관찰되었으나 경과관찰 하던 중, 생후 1개월경 흉골상부 함몰 및 흉부 함몰(chest retraction), 천명 악화 및 경구 수유량 감소로 타원에 내원하여 급성 기관지염 혹은 흡인성 폐렴 의증 하에 정맥항생제 치료를 받았다. 하지만, 증상이 호전되지 않아 소아 중환자실로 전원되었고, 상기도 협착증 의증 하에 시행한 컴퓨터전산화단층촬영에서 우측 후두개곡 낭종이 관찰되었다. 후두연화증의 확인을 위해 시행한 기관지 내시경 상, 후두개가 후방으로 접히면서 후두 입구쪽으로 전위되는 제 3형 후두연화증이었다. 상기도 폐쇄를 유발하는 후두개곡 낭종과 후두연화증의 개선을 위해 후두경 하 레이저를 이용하여 후두개곡 낭종의 제거 및 성문상부교정술 및 후두개고정술(epiglottopexy)을 시행하였다(Fig. 2). 수술 직후 기관 삽관을 제거하였고, 호흡의 악화 소견은 보이지 않았다. 이 후 호흡 및 연하 장애없이 경구 식이 가능하여 경과관찰 중이다.
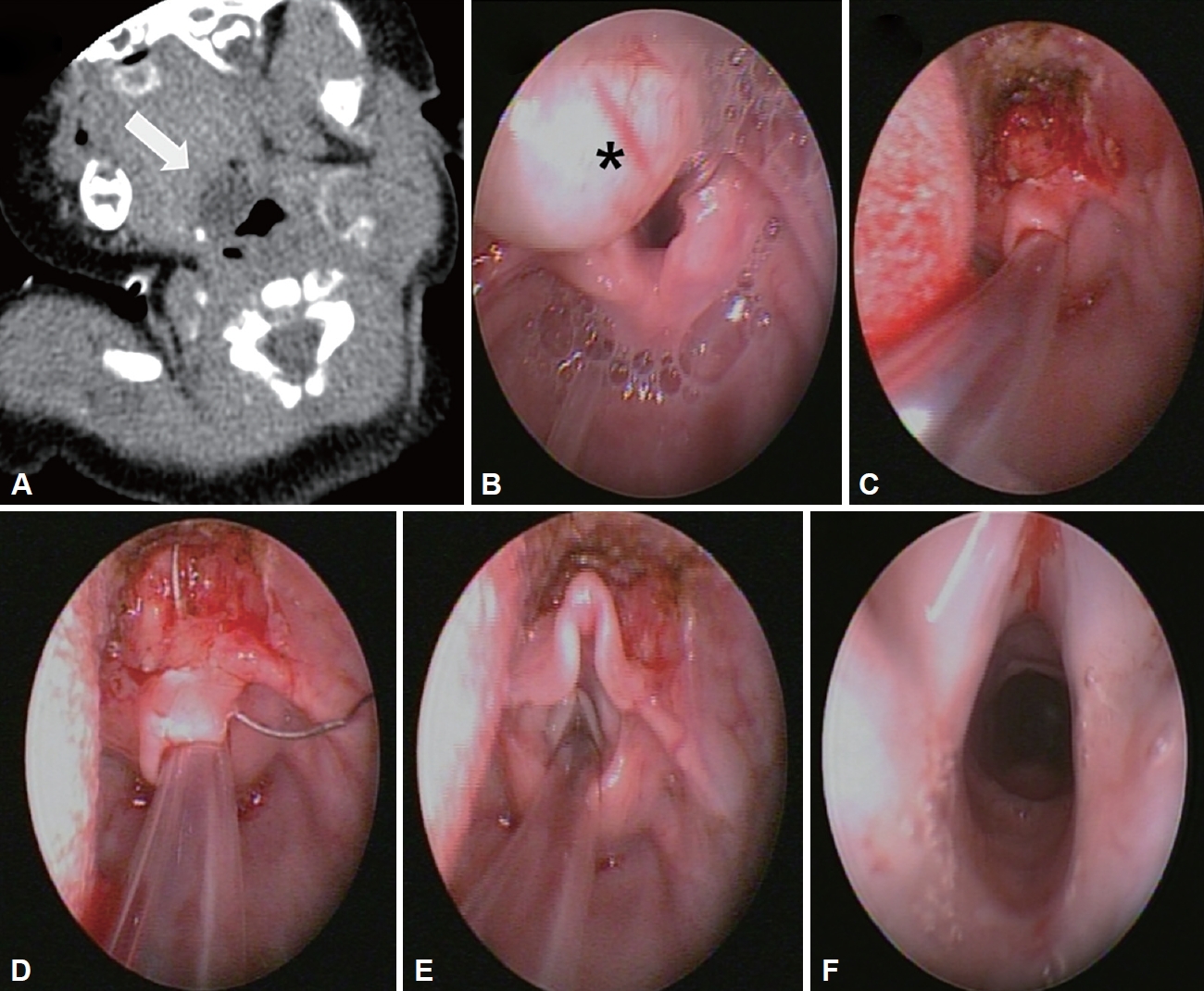
Case 2. Vallecular cyst excision and supraglottoplasty. A: CT showed 1.2×1 cm sized. Cystic lesion in the right vallecular fossa (white arrow). B: Endoscopic exam showed vallecular cyst (black asterisk) and laryngomalacia. C: Retroflexed epiglottis after vallecular cyst resection. D, E: Supraglottoplasy – epiglottopexy with PDS 3-0 suture. F: normal glottis and trachea.
고 찰
흡인성 천명은 영아에서 관찰되는 가장 흔한 후두연화증의 증상이다. 천명을 가진 환아의 60%는 후두연화증, 성대마비, 성문하 협착증, 혈종, 후두 낭종이며, 15%는 기도연화증이나 혈관 기형, 25%는 후비공폐쇄(choanal atresia), 얼굴 기형, 거대혀(macroglossia) 등이 원인이다. 그 중, 후두연화증은 신생아에서 발생하는 선천성 후두기형 중 가장 빈도가 높으며, 인후두 역류증이 동반되는 경우에는 증상이 더욱 악화될 수 있다. 따라서, 천명 및 연하곤란을 호소하는 환아들의 진단을 위해서 X-ray뿐 아니라 기도내시경, 전산화단층촬영 등을 사용하여 구조적 이상을 확인해 볼 수 있으며, 바륨삼킴검사(Modified Barium Swallow) 및 상부위장관조영술(Upper GastroIntestinal Series) 검사를 통해 위식도 역류질환의 동반 및 다른 연하곤란을 유발하는 원인이나 흡인 등의 문제는 없는지 확인하는 것이 추후 치료 방향에 영향을 미칠 수 있다[3]. 최근에는 내시경의 발달로 후두협착의 원인을 정확히 분석하여 성문상부 성형술이 필요한 환자들에게 적절한 외과적 치료를 시행하여, 보다 안전하고 효과적으로 치료를 할 수 있다.
후두연화증에 시행하는 내시경적 성문상부 성형술은 후두연화증의 종류에 따라 여러가지 방법이 있다. 본 증례에서는 후방 전위된 후두개를 전방으로 고정하여 기도를 확보하는 후두개고정술을 시행하였다. 수술 방법은 다음과 같다. 미세 겸자로 후두개를 잡아당겨 시야를 확보한 후, 후두개곡과 후두개가 맞닿는 부위의 점막을 레이저로 제거한다. 이후에 흡수성 봉합사(PDS 3-0)를 이용하여 후두개를 후두개곡에 고정하여 후두개를 전방 전위시켜 기도를 확보한다. 필요하면 짧아진 피열후두개주름에 의한 장력을 완화시키고 과잉의 피열연골 상부 조직을 제거하여, 함몰된 후두를 열어주면 호흡 곤란 증상 개선이 효과적으로 이루어질 수 있다[5,6].
후두개곡 낭종은 후두개 설측면에 투명한 액체를 가지는 다양한 크기의 단발성 낭종으로 발생한다. 임상적으로는 양성 낭종이나 위치 상 기도를 일부 막아 호흡곤란, 수유곤란, 흡기성 천명 등과 같은 증상을 유발하며, 이는 실제로 유아의 상기도 폐쇄와 사망의 원인으로도 알려져 있다[7,8]. 성인에서는 소아와 달리 대부분 우연히 발견되며, 감염 되어 낭종이 팽창하였을 경우 증상이 발생할 수 있다. 낭종의 진단을 위해 가장 먼저 고려되는 것은 굴절성 섬유 기관지경 검사이며, 단순 방사선 촬영과 초음파도 진단에 도움이 된다. 특히, 후두개곡 낭종의 확진은 기관지 내시경이나 후두경 검사로 할 수 있다[9]. 경구내 종물이 관찰되는 경우에 고려해 볼 수 있는 감별진단으로는 하마종, 혈관종, 갑상설관낭종, 표피양낭, 기형종, 설하 갑상선, 림프관종 등이 있다[10]. 낭종의 치료를 위해서는 내시경 하 레이저 절제술 혹은 조대술, 외부 절제술 등을 고려할 수 있다[11]. 이전 Burkart 등[12]의 연구에서는 내시경 경구 수술하는 것이 재발이나 합병증 없이 좋은 예후를 나타낸다고 보고하였으나, Zhang 등[13]의 연구에서는 내시경 하 조대술만 시행하는 것은 재발의 위험성이 있다고 보고하였다.
따라서, 후두개곡 낭종은 매우 드물지만, 연하곤란과 천명음과 같은 호흡곤란이 동반되는 경우에는 후두연화증 뿐 아니라 함께 고려해야 할 감별진단이다. 특히 진단이 지연되는 경우에는 생명의 위협이 될 수 있으므로 적절한 진단을 위해 노력해야 하며, 본 증례와 같이 기관지 내시경 혹은 굴절성 섬유 기관지경 검사가 도움이 될 것이다. 치료를 위해 후두경 및 내시경을 이용하여 절제술을 시행하여 기도를 확보하고, 동반된 후두연화증 및 역류성식도염을 함께 치료하는 것이 재발의 방지 및 적절한 치료를 위한 방법일 것이다.
Acknowledgements
None
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Authors’ Contribution
Conceptualization: HeeJung Kim, Nayeon Choi. Data curation: HeeJung Kim, Nayeon Choi. Formal analysis: HeeJung Kim, Nayeon Choi. Funding acquisition: HeeJung Kim, Nayeon Choi. Investigation: HeeJung Kim, Nayeon Choi. Methodology: HeeJung Kim, Nayeon Choi. Project administration: HeeJung Kim, Nayeon Choi. Resources: HeeJung Kim, Nayeon Choi. Software: HeeJung Kim, Nayeon Choi. Supervision: HeeJung Kim, Nayeon Choi. Validation: HeeJung Kim, Nayeon Choi. Visualization: HeeJung Kim, Nayeon Choi. Writing—original draft: HeeJung Kim, Nayeon Choi. Writing—review & editing: HeeJung Kim, Nayeon Choi. Approval of final manuscript: HeeJung Kim, Nayeon Choi.