ĒøäļæÉņĀäņĀüņČ£ņłĀ ĒÖśņ×ÉņŚÉņä£ ĒøäĻ░ü ņ×¼ĒÖ£
Abstract
Patients who undergo total laryngectomy often experience difficulties with their voice, olfaction, and taste due to the lack of airflow through nasal and oral cavities. While voice rehabilitation is more commonly performed, olfactory rehabilitation has gained importance in recent times with the use of various techniques. Previous studies have shown that incidence of hyposmia or anosmia (partial or total loss of smell) after total laryngectomy ranges from 25% to 100%. However, after olfactory rehabilitation, there has been notable improvement in olfaction, ranging from 46% to 88% of the patients. There are two main techniques for olfactory rehabilitation. The first involves creating airflow for smelling purposes by connecting the oral or nasal cavity to the tracheostoma using prosthetic laryngeal bypass devices. The second technique involves orofacial musculature training, which includes a nasal airflow-inducing maneuver known as the ŌĆ£polite yawning technique.ŌĆØ This maneuver creates negative pressure in the oropharynx, resulting in the induction of nasal airflow and potentially improving olfaction. Additionally, rehabilitation through biofeedback can facilitate airflow in the nasal cavity, further enhancing the sense of smell. In this review, we will introduce the principles, pathogenesis, and various techniques of olfactory rehabilitation, as well as summarize the outcomes of olfactory rehabilitation efforts.
Key words: Olfactory rehabilitation; Total laryngectomy; Laryngeal bypass devices; Nasal airflow inducing maneuver; Polite yawning
ņżæņŗ¼ ļŗ©ņ¢┤: ĒøäĻ░üņ×¼ĒÖ£; ĒøäļæÉņĀäņĀüņČ£ņłĀ; ĒøäļæÉ ņÜ░ĒÜī ņןņ╣ś; ļ╣äĻ░Ģ Ļ│ĄĻĖ░ ĒØÉļ”ä ņ£ĀļÅä ĻĖ░ļ▓Ģ; Ļ│ĄņåÉĒĢ£ ĒĢśĒÆł
ņä£ ļĪĀ
ĒøäļæÉņĀäņĀüņČ£ņłĀ(total laryngectomy)ņØä ļ░øņØĆ ĒÖśņ×ÉļōżņØĆ ĻĖ░ļÅäņÖĆ ņŗØļÅäĻ░Ć ļČäļ”¼ļÉśņ¢┤ ļ╣äĻ░ĢĻ│╝ ĻĄ¼Ļ░Ģņ£╝ļĪ£ Ļ│ĄĻĖ░Ļ░Ć ĒØÉļź┤ņ¦Ć ņĢŖĻĖ░ ļĢīļ¼ĖņŚÉ ņØīņä▒ļ┐É ņĢäļŗłļØ╝ ĒøäĻ░üĻ│╝ ļ»ĖĻ░üņŚÉ ņןņĢĀĻ░Ć ņāØĻĖ┤ļŗż[ 1]. ļīĆļČĆļČäņØś ĒÖśņ×ÉļōżņØĆ ĻĖ░Ļ┤ĆņŗØļÅäļłäĻ│Ą(Tracheoesophageal fistula, PROVOX TM, Atos Medical AB, Horby, Sweden)ņØ┤ļéś ņĀäņ×ÉĒøäļæÉļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņØīņä▒ņ╣śļŻīļź╝ ĒĢśņ¦Ćļ¦ī ĒøäĻ░ü ļ░Å ļ»ĖĻ░ü ņ×¼ĒÖ£ņØä ņĀüĻĘ╣ņĀüņ£╝ļĪ£ ļ░øļŖö ĒÖśņ×ÉļōżņØĆ ļō£ļ¼╝ļŗż. ĒøäļæÉņĀäņĀüņČ£ņłĀĻ│╝ Ļ┤ĆļĀ©ĒĢśņŚ¼ ļ░£ņä▒, ņé╝Ēé┤ĻĖ░ļŖź ļ░Å ĒÅÉĻĖ░ļŖź Ļ┤ĆļĀ© ņ×¼ĒÖ£ņØĆ ļŗżņ¢æĒĢ£ ņŚ░ĻĄ¼Ļ░Ć ļÉśņ¢┤ ņ׳ļŗż[ 2, 3]. ĒĢśņ¦Ćļ¦ī ĒøäĻ░ü ņ×¼ĒÖ£(olfactory rehabilitation)Ļ│╝ Ļ┤ĆļĀ©ļÉ£ ņŚ░ĻĄ¼ļŖö ļČĆņĪ▒ĒĢśļ®░, ņŗżņĀ£ ņ×äņāüņŚÉņä£ ļ¦ÄņØ┤ ņĀüņÜ®ļÉśĻ│Ā ņ׳ņ¦Ć ņĢŖļŗż. ĒøäĻ░ü ĻĖ░ļŖźņØĆ Ļ░ĆņŖż, ĒÖöņ×¼, ņāüĒĢ£ ņØīņŗØĻ│╝ Ļ░ÖņØĆ ņ£äĒŚś ņŗĀĒśĖļź╝ ņØĖņ¦ĆĒĢśĻ│Ā, ņ╣© ļČäļ╣ä, Ļ░ÉņĀĢ, ĻĖ░ņ¢Ą, ļ»ĖĻ░üņŚÉ Ļ┤ĆņŚ¼ĒĢ£ļŗż[ 4- 6]. ņØ┤ ļĢīļ¼ĖņŚÉ ĒøäĻ░ü ĻĖ░ļŖź ņĀĆĒĢśļŖö ņéČņØś ņ¦łņŚÉ ņśüĒ¢źņØä ņżĆļŗżļŖö ņŚ¼ļ¤¼ ļ│┤Ļ│ĀļōżņØ┤ ņ׳ļŗż[ 3, 7- 11]. ĒøäĻ░üņØś ņāØļ”¼ļŖö ĒøäĻ░üņŗĀĻ▓ĮņāüĒö╝ņäĖĒż(olfactory neuroepithelium)Ļ░Ć ņ×ÉĻĘ╣ļÉśņ¢┤ ļćīņŚÉņä£ ĒøäĻ░üņØä ņØĖņ¦ĆĒĢśļ®░, ĒøäĻ░üņØś Ļ▓ĮļĪ£ļŖö Ļ│ĄĻĖ░ ĒØÉļ”äņŚÉ ļö░ļØ╝ ņĀäļ╣äĻ░ĢņØä ĒåĄĒĢ£ Ļ▓ĮļĪ£(orthonasal way)ņÖĆ ĻĄ¼Ļ░ĢņØä Ļ▒░ņ│É Ēøäļ╣äĻ░ĢņØä ĒåĄĒĢ£ Ļ▓ĮļĪ£(retronasal way)Ļ░Ć ņ׳ļŗż[ 1, 12]. ļīĆļČĆļČäņØś ļ»ĖĻ░üņØĆ Ēøäļ╣äĻ░ĢņØä ĒåĄĒĢ£ Ļ▓ĮļĪ£ļĪ£ ņ¢╗ņ¢┤ņ¦Ćļ®░, ĒøäļæÉņĀäņĀüņČ£ņłĀ Ēøä ĒøäĻ░ü ņĀĆĒĢśļŖö ļ»ĖĻ░ü ņĀĆĒĢś ļ░Å ņŗØņÜĢ Ļ░ÉņåīļĪ£ ņØ┤ņ¢┤ņ¦äļŗż[ 13]. ĒøäļæÉņĀäņĀüņČ£ņłĀ Ēøä ĒøäĻ░ü ņĀĆĒĢśĻ░Ć ļ░£ņāØĒĢśļŖö ļ╣łļÅäļŖö 25%-100%ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż[ 3, 7, 14- 19]. Ļ░ü ņŚ░ĻĄ¼ļōżņŚÉņä£ ĒøäĻ░üņØä ĒÅēĻ░ĆĒĢśĻĖ░ ņ£äĒĢ┤ņä£ ņĮöļĪ£ ĒØĪņ×ģĒĢśļŖö ļ░®Ē¢ź(odorant) ļ¼╝ņ¦łņØ┤ļéś ĒØĪĻĖ░ ĒśĢĒā£ņØś ļ░®Ē¢źņĀ£(nebulizer odorance)ļź╝ ņé¼ņÜ®ĒĢśņśĆĻ│Ā, Ļ░ĢņĀ£ ĒØĪņ×ģ(forced inhalation)ņØä ĒĢśĻ▒░ļéś ņŻ╝Ļ┤ĆņĀüņØĖ ļ│┤Ļ│Ā(self-report), Ļ░ØĻ┤ĆņĀüņØĖ Ļ▓Ćņé¼ļĪ£ ĒøäĻ░ü Ļ▓Ćņé¼ ņŖżĒŗ▒(sniffin stick)ņØä ĒżĒĢ©ĒĢ£ ĒøäĻ░ü Ļ▓Ćņé¼ļź╝ ņØ┤ņÜ®ĒĢśņśĆļŗż[ 3, 7, 14- 19]. ņØ┤ļ¤░ Ļ▓Ćņé¼ ļ░®ļ▓ĢņØś ļŗżņ¢æņä▒ņ£╝ļĪ£ ĒøäļæÉņĀäņĀüņČ£ņłĀĒøä ĒøäĻ░ü ņĀĆĒĢś ļ░£ļ│æļźĀņØĆ ļŗżņ¢æĒĢśĻ▓ī ļ│┤Ļ│ĀļÉśņŚłļŗż. ļśÉĒĢ£, ĒøäļæÉņĀäņĀüņČ£ņłĀ Ēøä ĒøäĻ░ü ņ×¼ĒÖ£ņ╣śļŻīļź╝ ĒĢśļŖö Ļ▓ĮņÜ░ 46%-88%ņŚÉņä£ ĒøäĻ░üņØś Ļ░£ņäĀņØ┤ ņØ┤ļŻ©ņ¢┤ņĪīļŗż[ 7, 15, 20- 23]. ļ│Ė ņóģņäżņŚÉņä£ļŖö ĒøäļæÉņĀäņĀüņČ£ņłĀ ĒÖśņ×ÉļōżņŚÉĻ▓ī ļŗżņ¢æĒĢ£ ĒøäĻ░ü ņ×¼ĒÖ£ ļ░®ļ▓Ģ ļ░Å ņøÉļ”¼ļź╝ ņåīĻ░£ĒĢśĻ│Ā ĒøäĻ░ü ņ×¼ĒÖ£ņØś ņä▒Ļ│ĄļźĀņŚÉ ļīĆĒĢ┤ ņ×ÉņäĖĒ׳ ļŗżļŻ©ņ¢┤ļ│┤Ļ│Āņ×É ĒĢ£ļŗż.
ļ│Ė ļĪĀ
ĒøäļæÉņĀäņĀüņČ£ņłĀ ĒÖśņ×ÉņŚÉņä£ ĒøäĻ░ü ņĀĆĒĢśĻ░Ć ļ░£ņāØĒĢśļŖö ļ│æņØĖ
ĒøäļæÉņĀäņĀüņČ£ņłĀ Ēøä ĒøäĻ░ü ņĀĆĒĢśĻ░Ć ļ░£ņāØĒĢśļŖö ņØ┤ļĪĀņØĆ Ēü¼Ļ▓ī 2Ļ░Ćņ¦ĆļĪ£ ņäżļ¬ģĒĢĀ ņłś ņ׳ļŗż. ņ▓½ļ▓łņ¦Ė ņŻ╝ņÜö ņØ┤ļĪĀņØĆ ļ╣äĻ░Ģ ļé┤ Ļ│ĄĻĖ░ ĒØÉļ”äņØ┤ Ļ░ÉņåīĒĢśņŚ¼ ĒøäĻ░ü ņĀÉļ¦ēĻ╣īņ¦Ć ļ░®Ē¢ź ļ¼╝ņ¦łņØ┤ ļÅäļŗ¼ĒĢśĻĖ░ ņ¢┤ļĀĄĻ│Ā, ņØ┤ļŖö ĒøäĻ░üņŗĀĻ▓ĮņāüĒö╝ņäĖĒżņŚÉ ņĪ░ņ¦üĒĢÖņĀü ļ│ĆĒÖöļź╝ ņ£Āļ░£ĒĢśņŚ¼ ļ│Ćņä▒ņØ┤ ņØ╝ņ¢┤ļéśņä£ ĒøäĻ░ü ņĀĆĒĢśĻ░Ć ļ░£ņāØĒĢ£ļŗżļŖö Ļ▓āņØ┤ļŗż[ 24]. ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĒøäļæÉņĀäņĀüņČ£ņłĀņØä ļ░øņØĆ ĒÖśņ×ÉņŚÉĻ▓īņä£ ņä¼ļ¬©Ļ░Ć ņåīņŗżļÉśĻ│Ā, ļ»ĖĒåĀņĮśļō£ļ”¼ņĢä ņåÉņāüņØ┤ ļ░£ņāØĒĢśļ®░ ņĀÉņĢĪ ļČäļ╣ä ņäĖĒżĻ░Ć Ļ░ÉņåīĒĢśļŖö Ļ▓āņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż[ 25]. ļæÉļ▓łņ¦Ė ņØ┤ļĪĀņØĆ ĒøäļæÉņĀäņĀüņČ£ņłĀņØ┤ ĒøäļæÉņØś Ļ░ÉĻ░ü ņŗĀĻ▓ĮņØä ņåÉņāüņŗ£ņ╝£ ĒøäĻ░ü ņāüĒö╝ ļ░Å ņØĖĒøäļæÉ ņé¼ņØ┤ņŚÉ ļ░öņØ┤ņśżĒö╝ļō£ļ░▒ņØ┤ ņé¼ļØ╝ņ¦ĆĻĖ░ ļĢīļ¼ĖņØ┤ļØ╝ļŖö Ļ▓āņØ┤ļŗż[ 14].
ĒøäļæÉņĀäņĀüņČ£ņłĀ Ēøä ņ×¼ĒÖ£ ņ╣śļŻī ļ░®ļ▓Ģ
2000ļģäļīĆ ņØ┤ĒøäļČĆĒä░ ĒøäĻ░ü ņ×¼ĒÖ£ļÅä ņĀüĻĘ╣ņĀüņ£╝ļĪ£ Ē¢ēĒĢ┤ņ¦Ćļ®┤ņä£ ļŗżņ¢æĒĢ£ ņ×¼ĒÖ£ ĻĖ░ļ▓ĢļōżņØ┤ ņåīĻ░£ļÉśņŚłļŗż. ĒøäļæÉņĀäņĀüņČ£ņłĀ Ēøä ņ×¼ĒÖ£ ņ╣śļŻī ļ░®ļ▓ĢņØĆ Ēü¼Ļ▓ī 2Ļ░Ćņ¦ĆļĪ£ ļéśļłī ņłś ņ׳ļŗż. ļ╣äĻ░Ģ ļśÉļŖö ĻĄ¼Ļ░ĢĻ│╝ ĻĖ░Ļ┤ĆĻ│Ą(tracheostoma)ņØä ņØ╝ņŗ£ņĀüņ£╝ļĪ£ ņŚ░Ļ▓░ĒĢ┤ņŻ╝ņ¢┤ Ļ│ĄĻĖ░ ĒØÉļ”äņØä ļ¦īļōżņ¢┤ņŻ╝ļŖö ņØĖĻ│Ą ĒøäļæÉ ņÜ░ĒÜī ņןņ╣ś(prosthetic laryngeal bypass device)ņÖĆ ņĢłļ®┤ ļ░Å Ļ▓ĮļČĆ ĻĘ╝ņ£ĪļōżņØä ņé¼ņÜ®ĒĢśņŚ¼ ĻĄ¼ņØĖļæÉņŚÉ ņØīņĢĢņØä ņ£ĀļÅäĒĢśņŚ¼ Ļ│ĄĻĖ░ ĒØÉļ”äņØä ļ¦īļōżņ¢┤ņŻ╝ļŖö ĻĄ¼Ļ░ĢņĢłļ®┤ĻĘ╝ņ£Ī ĒøłļĀ©(orofacial musculature training)ņØ┤ ņ׳ļŗż[ 1, 26].
Ļ░ü ņ×¼ĒÖ£ ņ╣śļŻīņØś ļ░®ļ▓Ģ ļ░Å ņןļŗ©ņĀÉ
ĒøäļæÉ ņÜ░ĒÜī ņןņ╣ś( Fig. 1)ļŖö ĻĄ¼Ļ░ĢĻ│╝ ĻĖ░Ļ┤ĆĻ│ĄņØä ņØ╝ņŗ£ņĀüņ£╝ļĪ£ ņŚ░Ļ▓░ĒĢ┤ņŻ╝ļŖö Ļ░äļŗ©ĒĢ£ ĻĄ┤Ļ│ĪĒśĢ ĒŖ£ļĖīņØ┤ļŗż[ 1, 26- 31]. ĒŖ£ļĖīņØś ĒĢ£ņ¬ĮņØĆ ĻĖ░Ļ┤ĆĻ│ĄņØś ņ×ģĻĄ¼ļź╝ ļ¦ēĻ│Ā ļ░śļīĆņ¬Į ļüØņØĆ ņ×ģņłĀ ņé¼ņØ┤ņŚÉ ņ£äņ╣śĒĢśņŚ¼ ļ╣äĻ░Ģ ļ░Å ĻĄ¼Ļ░ĢĻ│╝ ĒĢśļČĆ ĻĖ░ļÅäļź╝ ņŚ░Ļ▓░ņŗ£ņ╝£ņżĆļŗż[ 1, 26]. ĒØĪĻĖ░ ņŗ£ ņĮö ņĢłņ£╝ļĪ£ Ļ│ĄĻĖ░ņØś ĒØÉļ”äņØ┤ ņāØĻĖ░ļ®┤ņä£ ļāäņāłļź╝ ļ¦ĪĻ▓ī ļÉ£ļŗż[ 1, 26]. ĒÖśņ×ÉļŖö ļ╣äņØĖļæÉļź╝ ļ¦ēņ¦Ć ņĢŖĻĖ░ ņ£äĒĢ┤ ņŚ░ĻĄ¼Ļ░£ļź╝ ņØ┤ņÖäņŗ£ĒéżļŖö ņŚ░ņŖĄņØä ĒĢ┤ņĢ╝ ĒĢ£ļŗż[ 1]. ņØ┤ ļ░®ļ▓ĢņØĆ ņēĮĻ│Ā ĒŖ╣ļ│äĒĢ£ ĒøłļĀ©ņØ┤ ĒĢäņÜöņŚåņ¦Ćļ¦ī ņØ╝ņāü ņāØĒÖ£ņŚÉņä£ ņ¦ĆņåŹņĀüņ£╝ļĪ£ ņé¼ņÜ®ņØ┤ ņ¢┤ļĀĄĻ│Ā ĻĖ░Ļ│äĻ░Ć Ēü¼ļ®░ ļ¼┤Ļ▓īĻ░Ć ņ׳ņ¢┤ ĻĖ░Ļ┤ĆĻ│ĄĻ│╝ ĻĄ¼Ļ░Ģņ£╝ļĪ£ ņןĻĖ░Ļ░ä Ļ│ĀņĀĢĒĢśņŚ¼ ņé¼ņÜ®ĒĢśĻĖ░Ļ░Ć ņ¢┤ļĀĄļŗż. ņØ┤ļĪ£ ņØĖĒĢ┤ ņŗżņÜ®ņĀüņØ┤ņ¦Ć ļ¬╗ĒĢśļŗżļŖö ļŗ©ņĀÉņØ┤ ņ׳ļŗż[ 16, 29]. Ļ│ĄņåÉĒĢ£ ĒĢśĒÆł(polite yawning)Ļ│╝ Ļ░ÖņØĆ ĻĄ¼Ļ░ĢņĢłļ®┤ĻĘ╝ņ£Ī ĒøłļĀ©( Fig. 2)ņØĆ ļ╣äĻ░ĢņØś Ļ│ĄĻĖ░ ĒØÉļ”äņØä ņ£ĀļÅäĒĢśļŖö ļ░®ļ▓Ģ(nasal airflow inducing maneuver)ņØ┤ļŗż[ 32]. Ļ▓ĮļČĆņÖĆ ņĢłļ®┤ ĻĘ╝ņ£ĪņØä ĒåĄĒĢ┤ ĻĄ¼ņØĖļæÉņŚÉ ņØīņĢĢņØä ĒśĢņä▒ĒĢśĻ│Ā ļ╣äĻ░ĢņØä ĒåĄĒĢ┤ Ļ│ĄĻĖ░ ĒØÉļ”äņØä ņ£ĀļÅäĒĢśļŖö ļ░®ļ▓Ģņ£╝ļĪ£ ņ×ģņłĀņØä ļČÖņØ┤Ļ│Ā ņŚ░ĻĄ¼Ļ░£ļŖö ņØ┤ņÖäņŗ£Ēéżļ®░, ĒĢśņĢģĻ│╝ ĻĄ¼Ļ░ĢņĀĆļŖö ņĢäļלļĪ£ ņØ┤ļÅÖĒĢśļÅäļĪØ ĒĢśņŚ¼ ĒĢśĒÆłņØä ĒĢśļŖö ļō»ĒĢ£ Ē¢ēļÅÖņØä ļ░śļ│ĄņĀüņ£╝ļĪ£ ĒĢśņŚ¼ ļāäņāłļź╝ ļ¦ĪļŖöļŗż[ 1, 15, 21, 33]. ĒśĖĒØĪņØĆ ĒĢśņĢģņØś ņÜ┤ļÅÖĻ│╝ ļÅÖņŗ£ņŚÉ ņØ╝ņ¢┤ļéśņä£ļŖö ņĢłļÉśļ®░ ņ░©ļČäĒĢ£ ņåŹļÅäļĪ£ ĒśĖĒØĪĒĢ£ļŗż. ņøĆņ¦üņ×äņØĆ Ļ░ĆļŖźĒĢśļ®┤ ņĀüņØĆ ļģĖļĀźņ£╝ļĪ£ ĒĢ┤ņĢ╝ ĒĢ£ļŗż[ 7]. ĻĄ¼Ļ░ĢņĢłļ®┤ĻĘ╝ņ£Ī ĒøłļĀ©ņØś ļ░®ļ▓ĢņØĖ Ļ│ĄņåÉĒĢ£ ĒĢśĒÆłņØś ĒÜ©Ļ│╝ņĀüņØĖ ņ×¼ĒÖ£ ļ░®ļ▓ĢņØĆ 3ļŗ©Ļ│äļĪ£ ņØ┤ļŻ©ņ¢┤ņ¦äļŗż. ņ▓½ļ▓łņ¦Ė ļŗ©Ļ│äļŖö ĒśĆņÖĆ ĻĄ¼Ļ░ĢņĀĆ, Ēä▒ņØ┤ ņĢäļלļĪ£ ĒĢśĻ░ĢĒĢśļ®┤ņä£ ļ╣ĀļźĖ ņØ┤ņÖäļÉ£ ņøĆņ¦üņ×äņØä ļ¦īļōĀļŗż[ 1, 15, 21, 33]. ļæÉļ▓łņ¦Ė ļŗ©Ļ│äļŖö ĒśĆ ļüØņØä ņ╣śņĪ░ļŖźņäĀ(alveolar ridge)ņŚÉ ņ£äņ╣śņŗ£ĒéżĻ│Ā ĒśĆļ┐īļ”¼ņÖĆ ĻĄ¼Ļ░ĢņĀĆļź╝ ņĢäļלļĪ£ ĒĢśĻ░ĢĒĢśļŖö ņ×æņØĆ ņøĆņ¦üņ×äņ£╝ļĪ£ ĒøäĻ░üņØä Ļ░£ņäĀņŗ£ĒéżļŖö Ļ▓āņØ┤ļŗż[ 6]. ņäĖļ▓łņ¦Ė ļŗ©Ļ│äļŖö ņĢĢļĀźĻ│äļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ļ░öņØ┤ņśżĒö╝ļō£ļ░▒( Fig. 3)ņØä ĒśĢņä▒ĒĢśļŖö Ļ▓āņØ┤ļŗż. ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ņŚÉņä£ ļ╣äĻ░Ģ ļé┤ Ļ│ĄĻĖ░ ĒØÉļ”äņØä ņ£ĀļÅäĒĢśļŖö ĒøłļĀ©ņØś ĒÜ©Ļ│╝ļź╝ ņ”ØĻ░Ćņŗ£ĒéżĻĖ░ ņ£äĒĢ┤ņä£ ļ░öņØ┤ņśżĒö╝ļō£ļ░▒ņØś ņØ┤ņĀÉņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż[ 22, 23, 34]. ņØ┤ļŖö ĒøäĻ░ü ņ×¼ĒÖ£ņØ┤ ņĀĢĒÖĢĒĢśĻ▓ī ņłśĒ¢ēļÉśļŖöņ¦Ć ĒÅēĻ░ĆĒĢĀ ņłś ņ׳ļŖö ļ░®ļ▓Ģņ£╝ļĪ£ ņĢĢļĀźĻ│äļŖö ĒĢ£ņ¬Į ņĮ¦ĻĄ¼ļ®ŹņŚÉ ņŚ░Ļ▓░ļÉśĻ│Ā ļ░śļīĆņ¬Į ņĮ¦ĻĄ¼ļ®ŹņØĆ ļ¦ēļŖöļŗż[ 6]. ņĀüņĀłĒĢ£ ņ×¼ĒÖ£ņØ┤ ļÉśļ®┤ ļ¼╝ņØś ņøĆņ¦üņ×äņØ┤ Ļ┤Ćņ░░ļÉśļ®░ ņŖżņŖżļĪ£ ļ░śļ│ĄļÉ£ ņŚ░ņŖĄņØä ĒåĄĒĢ┤ņä£ ĒøäĻ░ü ņ×¼ĒÖ£ņØś ļ░öņØ┤ņśżĒö╝ļō£ļ░▒ņØ┤ ĒśĢņä▒ļÉ£ļŗż[ 6]. ļ░öņØ┤ņśżĒö╝ļō£ļ░▒ņØä ĒåĄĒĢ£ ņ×¼ĒÖ£ļ▓ĢĻ│╝ Ļ░ÖņØĆ ļŗżņ¢æĒĢ£ ļ░®ļ▓ĢņØ┤ ļ╣äĻ░Ģņ£╝ļĪ£ Ļ│ĄĻĖ░ ĒØÉļ”äņØä ņ£ĀļÅäĒĢśņŚ¼ ļāäņāłļź╝ ļ¦ĪņØä ņłś ņ׳ļÅäļĪØ ļÅäņÖĆņżĆļŗż[ 6]. ņØ┤ļ¤¼ĒĢ£ Ļ│ĄņåÉĒĢ£ ĒĢśĒÆłņØä ĒåĄĒĢ£ ĒøäĻ░ü ņ×¼ĒÖ£ ļ░®ļ▓ĢņØä ņŗ£Ē¢ēĒĢĀņ¦Ć ņŚ¼ļČĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ņłśņłĀ ņĀä ĒÅēĻ░ĆĒĢśļŖö Ļ▓āņØ┤ ļÅäņøĆļÉ£ļŗż[ 6]. ļ¦īņĢĮ ņłśņłĀ ņĀä ĒøäĻ░ü ņןņĢĀĻ░Ć ņ׳ņŚłĻ▒░ļéś, ĻĄ¼Ļ░ĢņĢłļ®┤ ņøĆņ¦üņ×äņØä ņČ®ļČäĒ׳ ņŗ£Ē¢ēĒĢśļŖöļŹ░ ļŗżļźĖ ĒĢ┤ļČĆĒĢÖņĀüņØĖ ļ│ĆĒÖöĻ░Ć ņ׳ļŖö Ļ▓ĮņÜ░ ņØ┤ ļ░®ļ▓ĢņØ┤ ņĀüņĀłĒĢśņ¦Ć ņĢŖņØä ņłś ņ׳ļŗż[ 6, 35]. ņ”ē, Ļ░£ĻĄ¼ņŚÉ ņĀ£ĒĢ£ņØ┤ ņ׳ļŖö ĒÖśņ×Éļōż ļśÉļŖö ņØ┤ņĀäņØś Ļ▓ĮļČĆ Ļ│Įņ▓ŁņłĀ Ēøä ņ×ģĻ╝¼ļ”¼ ņøĆņ¦üņ×äņØ┤ ļ╣äļīĆņ╣ŁĒĢ£ Ļ▓ĮņÜ░ ĒÜ©Ļ│╝Ļ░Ć ņĀ£ĒĢ£ņØ┤ ļÉ£ļŗż[ 6, 35]. ļśÉ ļŗżļźĖ ĒøäĻ░ü ņ×¼ĒÖ£ ļ░®ļ▓Ģņ£╝ļĪ£ ļ╣äĻ░ĢņŚÉ Ļ│ĄĻĖ░ļź╝ Ļ░ĢĒĢśĻ▓ī ļČłņ¢┤ļäŻņØīņ£╝ļĪ£ņŹ© ļāäņāłļź╝ ļ¦ĪņØä ņłś ņ׳ļŗżļŖö ņØ┤ļĪĀņŚÉņä£ ņŗ£ņ×æļÉ£ Rogers ĒåĄĻĖ░ļ▓ĢņØ┤ ņ׳ņ£╝ļéś ņØ┤ ļ░®ļ▓ĢņØĆ Ēü░ ņŻ╝ļ¬®ņØä ļ░øņ¦Ć ļ¬╗Ē¢łļŗż[ 36].
ĒøäĻ░ü ņ×¼ĒÖ£ņØś ĒÜ©Ļ│╝ ļ░Å ņä▒Ļ│ĄļźĀ
Ļ│ĄņåÉĒĢ£ ĒĢśĒÆłĻ│╝ Ļ░ÖņØĆ ļ╣äĻ░ĢņØś Ļ│ĄĻĖ░ ĒØÉļ”äņØä ņ£ĀļÅäĒĢśļŖö ĻĖ░ļ▓ĢņØä ņØ┤ņÜ®ĒĢ£ ĒøäĻ░ü ņ×¼ĒÖ£ņØĆ ĒÜ©Ļ│╝Ļ░Ć ļ╣äĻĄÉņĀü ņóŗņĢśļŗż( Table 1). ņØ┤ ļ░®ļ▓ĢņØĆ ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ļōżņØä ĒåĄĒĢ┤ ļåÆņØĆ ĻĘ╝Ļ▒░ ņłśņżĆ(level I evidence status)ņØä ņ¢╗ņŚłĻ│Ā ņ£Āļ¤ĮņØś ņŚ¼ļ¤¼ ĻĄŁĻ░ĆņŚÉņä£ ĒøäĻ░ü ņ×¼ĒÖ£ņØś ļ░®ļ▓Ģņ£╝ļĪ£ ļäÉļ”¼ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŗż[ 20- 22, 33, 37, 38]. Ļ│ĄņåÉĒĢ£ ĒĢśĒÆł ļ░®ņŗØņØä ĒåĄĒĢ£ ĒøäĻ░ü ņ×¼ĒÖ£ņØĆ ņĀäļ¼ĖĻ░ĆņØś ņ¦ĆļÅäļź╝ ļ░øņØä ļĢīņÖĆ ņ¦æņŚÉņä£ ĒÖśņ×É ņŖżņŖżļĪ£ ņŚ░ņŖĄĒĢĀ ļĢī ļ¬©ļæÉ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłņ£╝ļéś, ĒŖ╣Ē׳ ņĀäļ¼ĖĻ░ĆņØś ļÅäņøĆņØä ļ░øņØä ļĢī Ļ▓░Ļ│╝Ļ░Ć ļŹö ņóŗņĢśļŗż[ 22]. ņĀäļ¼ĖĻ░ĆņØś 30ļČä ņĀĢļÅäņØś ņ×¼ĒÖ£ ĻĄÉņ£Ī ņäĖņģśĻ│╝ ņ×ÉĻ░Ć ĒøłļĀ©ņØä ĒåĄĒĢ┤ņä£ ĒÜ©Ļ│╝ņĀüņØĖ ĒøäĻ░ü Ļ░£ņäĀņØ┤ ļ│┤ņśĆļŗż. ļśÉĒĢ£, ņØ┤ņĀä ņŚ░ĻĄ¼ņŚÉņä£ ĒøäļæÉ ņÜ░ĒÜī ņןņ╣śļź╝ ņØ┤ņÜ®ĒĢ£ ņ×¼ĒÖ£ ļ░®ļ▓ĢņØ┤ ĒøäļæÉņĀäņĀüņČ£ņłĀ ĒÖśņ×ÉņŚÉĻ▓ī ņĀĢņāüņØĖĻ│╝ ļ╣äņŖĘĒĢ£ Ļ│ĄĻĖ░ ĒØÉļ”äņØä ņāØņé░ĒĢ£ļŗżļŖö Ļ▓āņØ┤ ņ”Øļ¬ģļÉśņŚłĻ│Ā, ņØ┤ļŖö ĒøäĻ░ü ļŖźļĀźĻ│╝ ņ¢æņØś ņāüĻ┤ĆĻ┤ĆĻ│äļź╝ Ļ░ĆņĪīļŗż[ 27, 31, 39]. ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ļōżņØ┤ ĒøäļæÉ ņÜ░ĒÜī ņןņ╣śļź╝ ņØ┤ņÜ®ĒĢ£ ĒøäĻ░ü ņ×¼ĒÖ£ņØ┤ ĒøäļæÉņĀäņĀüņČ£ņłĀ ĒÖśņ×ÉņŚÉĻ▓īņä£ ĒøäĻ░üņØś ņĀĢĒÖĢņä▒ņØä ņ”ØĻ░Ćņŗ£Ēé©ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż[ 27, 28, 31, 40].
Ļ▓░ ļĪĀ
ĒøäļæÉņĀäņĀüņČ£ņłĀ Ēøä ĒøäĻ░ü ņĀĆĒĢś ļ░Å ņ×¼ĒÖ£ņŚÉ ļīĆĒĢ┤ Ļ┤Ćņŗ¼ņØ┤ ņĀüĻ│Ā ņŚ░ĻĄ¼ļÉ£ ļ░öĻ░Ć ļČĆņĪ▒ĒĢśļŗż. ĻĘĖļ¤¼ļéś, ĒøäĻ░üņØĆ ļ»ĖĻ░üņØä ĒżĒĢ©ĒĢ£ ĒÖśņ×ÉļōżņØś ņéČņØś ņ¦łņŚÉ ņ¦ĆļīĆĒĢ£ ņśüĒ¢źņØä ņżĆļŗż. ĒøäĻ░ü ņ×¼ĒÖ£ņØĆ 30ļČä ņĀĢļÅäņØś ĻĄÉņ£Īņ£╝ļĪ£ ņä▒Ļ│ĄņĀüņØĖ ņ×¼ĒÖ£ņØ┤ ļÉĀ ņłś ņ׳ņ£╝ļ»ĆļĪ£, ĒøäļæÉņĀäņĀüņČ£ņłĀ ĒÖśņ×ÉļōżņŚÉĻ▓īņä£ ĒøäĻ░ü ņ×¼ĒÖ£ņŚÉ ļīĆĒĢ£ ņżæņÜöņä▒ņØ┤ ņØĖņ¦ĆļÉśņ¢┤ņĢ╝ ĒĢĀ Ļ▓āņ£╝ļĪ£ ņé¼ļŻīļÉ£ļŗż.
Fig.┬Ā1.
Olfactory rehabilitation using prosthetic laryngeal bypass devices. 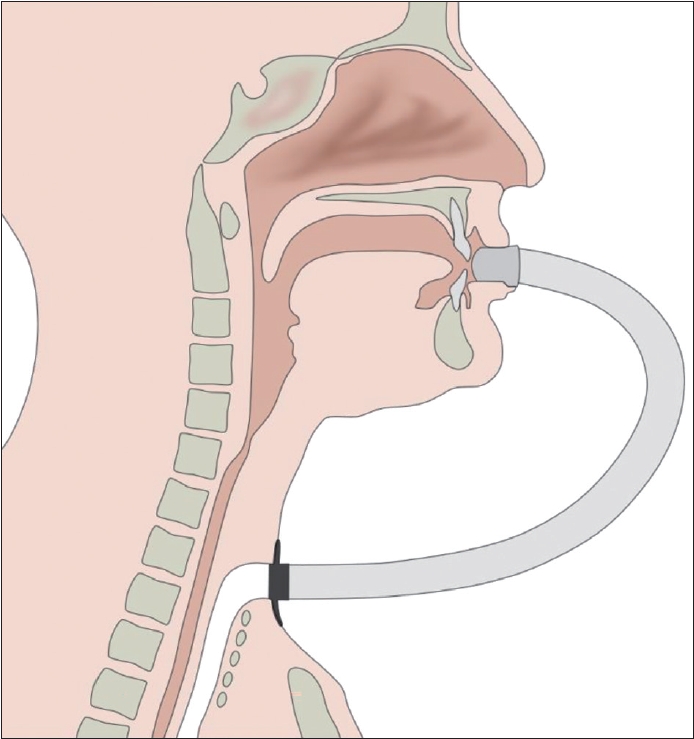
Fig.┬Ā2.
Olfactory rehabilitation using nasal airflow inducing maneuver (polite yawning technique). Black arrows indicates nasal airflow. White arrows indicates downward movement of mouth floor during polite yawning technique. 
Fig.┬Ā3.
Biofeedback using water manometer and evaluation during training. Black arrow indicates movement of water during training. 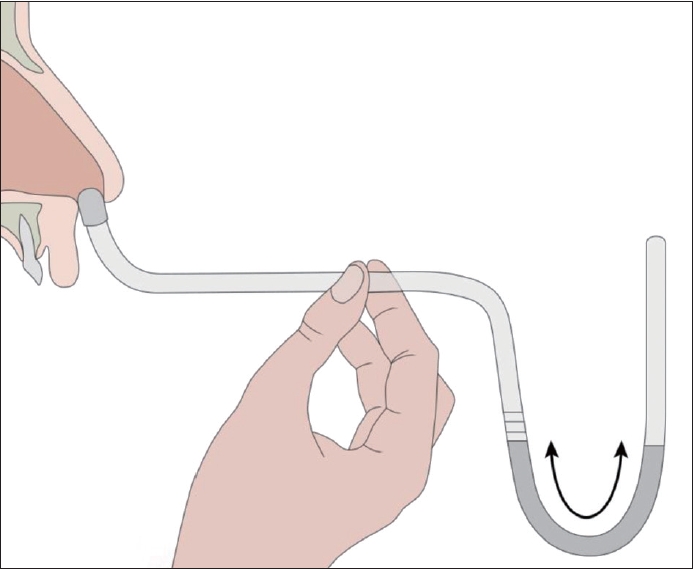
Table┬Ā1.
Outcomes of olfactory rehabilitation using nasal airflow inducing maneuver
|
Rehabilitation |
Time and duration |
Outcomes (incidence of olfactory dysfunction) |
|
Hilgers et al. [7] |
HP |
HP after one 30 minutes session |
75% ŌåÆ 43% |
|
Risberg-Berlin et al. [23] |
CS+HP |
Weekly 30 minutes sessions 6 weeks |
58% ŌåÆ 21% |
|
Ward et al. [22] |
CS vs. HP |
HP: One session |
HP: 65% ŌåÆ 20% |
|
CS: Weekly 30 minutes session 5 weeks |
CS: 85% ŌåÆ 25% |
|
Haxel et al. [20] |
HP |
One 30 minutes session |
72% ŌåÆ 24% |
REFERENCES
1. Moor JW, Rafferty A, Sood S. Can laryngectomees smell? Considerations regarding olfactory rehabilitation following total laryngectomy. J Laryngol Otol 2010; 124( 4): 361- 5.   2. Johnson JT, Casper J, Lesswing NJ. Toward the total rehabilitation of the alaryngeal patient. Laryngoscope 1979; 89( 11): 1813- 9. 3. Ackerstaff AH, Hilgers FJ, Aaronson NK, Balm AJ. Communication, functional disorders and lifestyle changes after total laryngectomy. Clin Otolaryngol Allied Sci 1994; 19( 4): 295- 300. 4. Varga EK, Breslin PA, Cowart BJ. The impact of chemosensory dysfunction on quality of life. Chem Senses 2000;25:654.
5. Hufnagl B, Lehrner J, Deecke L. Development of a questionnaire for the assessment of self reported olfactory functioning. Chem Senses 2003;28:E27.
6. Ward E, Rumbach A, van As-Brooks CJ. Olfaction following total laryngectomy. J Laryngol Voice 2012; 2( 1): 10- 20. 7. Hilgers FJ, van Dam FS, Keyzers S, Koster MN, van As CJ, Muller MJ. Rehabilitation of olfaction after laryngectomy by means of a nasal airflow-inducing maneuver: the ŌĆ£polite yawningŌĆØ technique. Arch Otolaryngol Head Neck Surg 2000; 126( 6): 726- 32. 8. Hilgers FJ, Ackerstaff AH, Aaronson NK, Schouwenburg PF, Van Zandwijk N. Physical and psychosocial consequences of total laryngectomy. Clin Otolaryngol Allied Sci 1990; 15( 5): 421- 5. 9. Miwa T, Furukawa M, Tsukatani T, Costanzo RM, DiNardo LJ, Reiter ER. Impact of olfactory impairment on quality of life and disability. Arch Otolaryngol Head Neck Surg 2001; 127( 5): 497- 503. 10. Deems DA, Doty RL, Settle RG, Moore-Gillon V, Shaman P, Mester AF, et al. Smell and taste disorders, a study of 750 patients from the University of Pennsylvania Smell and Taste Center. Arch Otolaryngol Head Neck Surg 1991; 117( 5): 519- 28. 11. Tennen H, Affleck G, Mendola R. Coping with smell and taste disorders. In: Getchell TV, Bartoshuk LM, Doty RL, Snow JB, editors. Smell and Taste in Health and Disease. New York: Raven Press;1991. p.787-802.
12. Leon EA, Catalanotto FA, Werning JW. Retronasal and orthonasal olfactory ability after laryngectomy. Arch Otolaryngol Head Neck Surg 2007; 133( 1): 32- 6. 13. Henkin RI, Smith FR. Hyposmia in acute viral hepatitis. Lancet 1971; 1( 7704): 823- 6. 14. Henkin RI, Hoye RC, Ketcham AS, Gould WJ. Hyposmia following laryngectomy. Lancet 1968; 292( 7566): 479- 81. 15. Hilgers FJ, Jansen HA, Van As CJ, Polak MF, Muller MJ, Van Dam FS. Long-term results of olfaction rehabilitation using the nasal airflow-inducing (ŌĆ£polite yawningŌĆØ) maneuver after total laryngectomy. Arch Otolaryngol Head Neck Surg 2002; 128( 6): 648- 54. 16. Van Dam FS, Hilgers FJ, Emsbroek G, Touw FI, Van As CJ, de Jong N. Deterioration of olfaction and gustation as a consequence of total laryngectomy. Laryngoscope 1999; 109( 7 Pt 1): 1150- 5. 17. Welge-Luessen A, Kobal G, Wolfensberger M. Assessing olfactory function in laryngectomees using the SniffinŌĆÖSticks test battery and chemosensory evoked potentials. Laryngoscope 2000; 110( 2 Pt 1): 303- 7.  18. Ritter FN. Fate of olfaction after laryngectomy. Arch Otolaryngol 1964; 79( 2): 169- 71. 19. Henkin RI, Larson AL. On the mechanism of hyposmia following laryngectomy in man. Laryngoscope 1972; 82( 5): 836- 43. 20. Haxel BR, Fuchs C, Fruth K, Mann WJ, Lippert BM. Evaluation of the efficacy of the ŌĆśnasal airflow-inducing manoeuvreŌĆÖ for smell rehabilitation in laryngectomees by means of the SniffinŌĆÖ Sticks test. Clin Otolaryngol 2011; 36( 1): 17- 23. 21. Risberg-Berlin B, M├Čller RY, Finizia C. Effectiveness of olfactory rehabilitation with the nasal airflow-inducing maneuver after total laryngectomy: one-year follow-up study. Arch Otolaryngol Head Neck Surg 2007; 133( 7): 650- 4. 22. Ward E, Coleman A, van As-Brooks C, Kerle S. Rehabilitation of olfaction post-laryngectomy: a randomised control trial comparing clinician assisted versus a home practice approach. Clin Otolaryngol 2010; 35( 1): 39- 45. 23. Risberg-Berlin B, Ylitalo R, Finizia C. Screening and rehabilitation of olfaction after total laryngectomy in Swedish patients: results from an intervention study using the nasal airflow-inducing maneuver. Arch Otolaryngol Head Neck Surg 2006; 132( 3): 301- 6. 24. Miani C, Ortolani F, Bracale AM, Petrelli L, Staffieri A, Marchini M. Olfactory mucosa histological findings in laryngectomees. Eur Arch Otorhinolaryngol 2003; 260( 10): 529- 35. 25. Fisher EW, Lund VJ, Rutman A. The human nasal mucosa after deprivation of airflow: a study of laryngectomy patients. Rhinology 1992; 30( 1): 5- 10. 26. Rosa VM, Fores JML, da Silva EPF, Guterres EO, Marcelino A, Nogueira PC, et al. Interdisciplinary interventions in the perioperative rehabilitation of total laryngectomy: an integrative review. Clinics (Sao Paulo) 2018; 73( suppl 1): e484s.  27. Mozell MM, Hornung DE, Leopold DA, Youngentob SL. Initial mechanisms basic to olfactory perception. Am J Otolaryngol 1983; 4( 4): 238- 45. 28. Schwartz DN, Mozell MM, Youngentob SL, Leopold DL, Sheehe PR. Improvement of olfaction in laryngectomized patients with the larynx bypass. Laryngoscope 1987; 97( 11): 1280- 6. 29. G├Čktas O, Fleiner F, Paschen C, Lammert I, Schrom T. Rehabilitation of the olfactory sense after laryngectomy: long-term use of the larynx bypass. Ear Nose Throat J 2008; 87( 9): 528- 30. 30. Brusis T. [A smelling prosthesis for laryngectomized patients]. Laryngol Rhinol Otol (Stuttg) 1985; 64( 6): 309- 10 German. 31. Tatchell RH, Lerman JW, Watt J. Olfactory ability as a function of nasal air flow volume in laryngectomees. Am J Otolaryngol 1985; 6( 6): 426- 32. 32. van der Molen L, Kornman AF, Latenstein MN, van den Brekel MW, Hilgers FJ. Practice of laryngectomy rehabilitation interventions: a perspective from Europe/the Netherlands. Curr Opin Otolaryngol Head Neck Surg 2013; 21( 3): 230- 8. 33. Manestar D, Ti─ćac R, Mari─Źi─ć S, Malvi─ć G, ─īorak D, Marjanovi─ć Kavanagh M, et al. Amount of airflow required for olfactory perception in laryngectomees: a prospective interventional study. Clin Otolaryngol 2012; 37( 1): 28- 34. 35. van As-Brooks CJ, Finizia CA, Kerle SM, Ward EC. Rehabilitation of olfaction and taste following total laryngectomy. In: Ward EC, van As-Brooks CJ, editors. Head and Neck Cancer: Treatment, Rehabilitation, and Outcomes. San Diego, CA: Plural Publishing;2014. p.421-45.
36. Gilchrist AG. Rehabilitation after laryngectomy. Acta Otolaryngol 1973; 75( 6): 511- 8. 37. Risberg-Berlin B, Ryd├®n A, M├Čller RY, Finizia C. Effects of total laryngectomy on olfactory function, health-related quality of life, and communication: a 3-year follow-up study. BMC Ear Nose Throat Disord 2009; 9: 8. 38. M├│ricz P, Kiss P, Somogyv├Īri K, Aradi M, Gerlinger I. Objective assessment of olfactory rehabilitation after laryngectomy. Clin Otolaryngol 2011; 36( 5): 518- 9. 39. Moore-Gillon V. The nose after laryngectomy. J R Soc Med 1985; 78( 6): 435- 9. 40. Mozell MM, Schwartz DN, Youngentob SL, Leopold DA, Hornung DE, Sheehe PR. Reversal of hyposmia in laryngectomized patients. Chem Senses 1986; 11( 3): 397- 410.
|
|











