서 론
후두골격수술(laryngeal framework surgery)은 후두의 골격인 연골과 근육을 변화시켜서 성대의 위치와 긴장을 교정하는 수술이다. 성대마비는 갑상선수술, 흉부수술, 기도삽관, 종양의 침습, 특발성(idiopathic) 등 다양한 원인에 의하여 되돌이후두신경의 손상이 발생하고, 이로 인해 동측의 성대 움직임이 제한되는 질환이다. 한쪽의 성대 움직임이 제한되면 발성 시 성문틈이 발생하고 단위시간당 성문틈 사이로 통과하는 기류량이 증가하여 기식음이 특징이 되는 발성장애가 나타난다[1]. 후두골격수술은 고정된 성대를 내전시켜 정상측 성대와의 접촉을 가능하게 하여 기식음을 제거하고 음성을 향상시킬 수 있다. 일측성 성대마비에 사용되는 후두골격수술에는 제 1형 갑상성형술(type 1 thyroplasty), 피열연골내전술(arytenoids adduction), 내전성 피열연골견인술(adductive arytenopexy) 등이 있다[2]. 제 1형 갑상성형술과 피열연골내전술은 Isshiki에 의해 1974-1976에 걸쳐 집대성된 이후 널리 시행되고 있다[3]. 내전성 피열연골견인술은 1998년 Zeitels 등[4]에 의해 소개되었으며 미국의 일부 그룹에서만 시행되고 있다. 이번 연구에서는 일측성 성대마비에 대한 전통적 수술방법인 후두골격수술 각각의 특징과 수술 시 주의할 점을 정리하였으며, 최근 보고된 변형된 수술 방법을 문헌 고찰을 통해 알아보고자 한다.
본 론
후두의 골격구조
성대운동은 상후두신경(superior laryngeal nerve, SLN)과 되돌이후두신경(recurrent laryngeal nerve, RLN)의 지배를 받는 후두내재근(laryngeal intrinsic muscle)의 운동으로 이루어진다. 후윤상피열근(posterior cricoarytenoid muscle, PCAM)은 유일한 후두외전근으로 피열연골의 근육돌기에서 윤상연골 후면으로 넓게 이어져 있다. 성대를 내전시키는 근육에는 피열사이근(interarytenoid muscle, IAM), 외윤상피열근(lateral cricoarytenoid muscle, LCAM), 갑상피열근(thyroarytenoid muscle, TAM) 등이 있다. 이들 중 LCAM이 가장 강력한 내전근이며 근돌기에서 윤상연골 상연을 향해 전하방으로 수축하여 성대를 내측으로 회전(rotation) 시키는 역할을 한다. TAM은 내전기능과 함께 긴장도를 높이는 기능을 하며, IAM은 양측의 피열연골을 서로 내측으로 당기는 기능을 한다. IAM은 양측에서 RLN의 운동지배를 받는다. 윤상갑상근(cricothyroid muscle)은 갑상연골을 하방으로 당겨서 성대의 길이를 길어지게 하여 긴장도를 높이며, 후두내재근 중 유일하게 SLN의 운동지배를 받는다. 후두골격 수술은 이 근육들의 기능을 강화 또는 억제시키는 방향으로 고안되었다. 이때 피열연골의 움직임은 여러 후두내재근이 동시에 작용하며 내전, 외전뿐만 아니라 활공(sliding)과 로킹(rocking) 운동도 동시에 일어난다.
제 1형 갑상성형술(Type 1 thyroplasty)
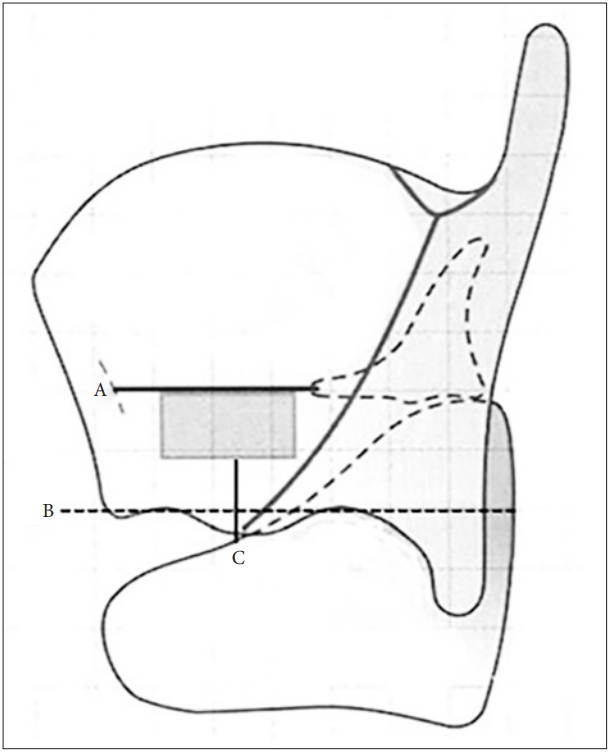
제 1형 갑상성형술은 1974년 Isshiki에 의해 개발된 이후 일측성 성대마비환자의 성문폐쇄부전을 교정하기 위한 수술방법으로 널리 사용되었다. 수술 전 양측 갑상연골을 압박해서 효과를 예측할 수 있다. 수술방법은 피부를 절개하고 피부 피판을 올려서 갑상연골을 노출시킨다. 갑상연골의 연골막을 올리고 갑상연골에 삽입 창을 만든 후 성대 내전을 위한 보형물을 삽입한다. 삽입되는 보형물로는 실리콘 블럭(silicon block)이 주로 사용되며, 이는 술자가 직접 원하는 모양으로 깍아(carbing)서 사용한다[5]. 그 외에 hydroxyapatite 제품으로 각각의 크기가 미리 만들어져서 제공되는 VoCom (Smith & Nephew Richards, Inc., Memphis, TN, USA), 또는 특정한 크기나 모양이 없는 Gore-Tex ribbon, titanium plate도 사용되지만 현재 국내에서는 시판되지 않는다[5-8]. 수술에서 성대의 위치에 맞게 갑상연골에 삽입 창을 만드는 것이 중요하다(Fig. 1). 갑상연골의 전연각이 남자가 여자보다 예각이기 때문에 정중선에서 남자는 7 mm 정도 뒤, 여자는 5 mm 정도 뒤에서 대략 가로 10 mm, 세로 5 mm의 직사각형 갑상연골창을 도안한다. 성대 전연합부의 위치는 갑상연골 정중선의 중간점으로 알려져 있다. 이 위치에서 갑상연골 창의 윗변(upper surface)이 성대 자유연에 평행하게 위치하도록 주의해야 하며, 이를 위해 갑상연골의 하연(lower edge)을 충분히 노출하여 연골 하연에 평행하게 연골 창의 윗변을 도안한다. 이때 갑상연골 하연의 돌출부로 인해 방향이 왜곡되지 않도록 주의한다. 또한 갑상연골 창의 밑변과 갑상연골 하연 사이에 최소한 3 mm의 연골 지주(cartilage strut)를 남김으로써 연골이 부서지는 것을 방지한다(Fig. 1).
피열연골내전술(Arytenoid adduction)
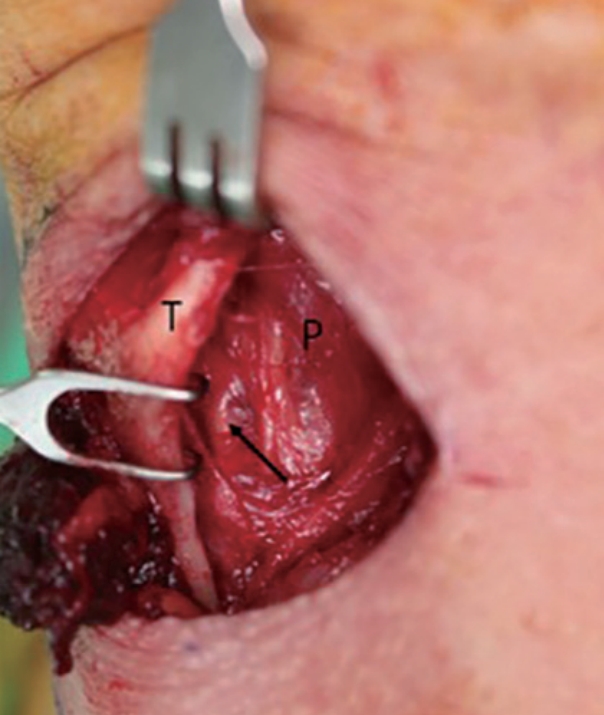
피열연골내전술의 원리는 가장 강력한 내전근인 LCAM의 수축 방향으로 피열연골의 근돌기를 견인하여 피열연골의 성대돌기를 내회전시키고 위상을 조정하는 효과를 얻는 것이다. 피열연골내전술의 적응증이 명확히 정해진 것은 없지만 큰 후성문틈이 있거나, 양측 성대의 위상 차이가 있을 때, 또는 최대발성시간이 5초 이하인 경우에 필요한 것으로 알려져 있다[9-11]. 수술 방법은 경부절개 후 피부피판을 올리고 인두수축근을 갑상연골 후연에서 절개한다. 갑상연골의 내측 연골막을 안쪽으로 박리하면서 연결된 이상와 점막을 후방으로 박리하면 후두내재근과 근돌기가 노출된다(Fig. 2). 수술의 포인트는 피열연골의 근돌기를 찾는 것인데 윤상갑상관절(cricothyroid joint)에서 윤상연골을 상연을 따라가면 윤상피열관절(cricoarytenoid joint)을 찾을 수 있고, 여기에서 상방 1 cm 범위 내에 쌀알 형태의 피열연골 근돌기를 촉지하여 찾을 수 있다. 피열연골에 비흡수성 봉합사를 이용하여 8자 형태의 봉합 후 실의 양측 끝을 갑상연골의 앞쪽으로 견인하여 묶어준다. 수술 중 이상와 공간의 노출을 향상시키기 위해 Issiki는 윤상갑상관절을 분리하였지만 갑상연골의 후연을 부분적으로 절제하여 시야를 좋게 하는 방법도 시행된다[12,13].
피열연골견인술(Arytenopexy)
피열연골내전술이 LCAM의 근수축을 모방한 수술방법인 것에 비하여 피열연골견인술은 피열연골의 운동에 영향을 미치는 TAM, PCAM, IAM 등과 같은 여러 후두내전근의 다양한 효과를 동시에 구현하고자 고안되었다[14]. 접근법은 피열연골내전술과 유사하며 윤상갑상관절을 분리시킨 후 윤상피열관절을 분리시켜서 관절면을 노출시키고 윤상피열관절면과 피열연골을 관통하는 봉합을 시행함으로써 피열연골을 내측으로 내전 및 로킹 시키는 효과를 얻고자 하였다. 피열연골견인술은 제 1형 갑상성형술이나 피열연골내전술 처럼 널리 시행되지는 않으며 주로 하버드 계열에서 시행되고 있다. 수술결과에 대한 많은 보고가 있는 것은 아니지만 피열연골견인술 후 최대발성시간이 증가하고 음강도가 강화되었으며 평균호기류율이 감소하였다는 보고가 있다[15].
후두골격수술의 새로운 시도
여러 연구를 통해 후두골격수술이 성대마비 환자의 음성 향상에 유용하다는 것이 밝혀졌지만, 수술 술기의 난이도와 경부절개로 인한 반흔 등의 문제점이 있으며, 최근 이를 보완하기 위한 다양한 시도들이 보고되었다.
경구강 피열연골내전술(Transoral arytenoid adduction)
미세후두수술에서 사용되는 현수후두경을 이용하여 후두에 접근한다. 이산화탄소 레이저를 이용하여 피열연골의 점막을 절개하고 근돌기를 노출시킨 후 봉합사를 건다. 전경부의 최소절개를 통해 척추바늘을 후두로 삽입한 후 이를 통해 봉합사를 전경부로 견인하여 묶어 줌으로써 피열연골을 내회전시킨다[16].
경구강 실리콘 내전술(Transoral silastic medializatin)
현수후두경 접근법을 이용하여 마비된 성대의 상후두에 점막을 절개한다. 부성문공간(paraglottic space)을 박리 후 실리콘 블록을 삽입하고 고정한다. 보고에 의하면 22명의 환자에서 수술 시행 후 1년 동안 추적관찰 하였을 때 음성장애지수-10, 음성관련삶의질평가, GRBAS 스케일, 최대발성시간, 연하장애척도평가 등에서 모두 유의한 향상을 보였다[17].
내시경 피열연골 내전술(Endoscopic arytenoid medialization)
현수후두경 접근법을 통하여 마비된 성대의 피열연골 외측과 부성문공간에 지방을 주입함으로써 피열연골과 성대의 내전 효과를 기대한다. 보고에 의하면 17명의 환자에서 수술 시행 후 1년 동안 추적관찰 하였을 때 최대발성시간, 주파수변동율, 진폭변동율, 조화음대잡음비 등이 유의하게 향상되었다[18].
후두골격수술의 장단점
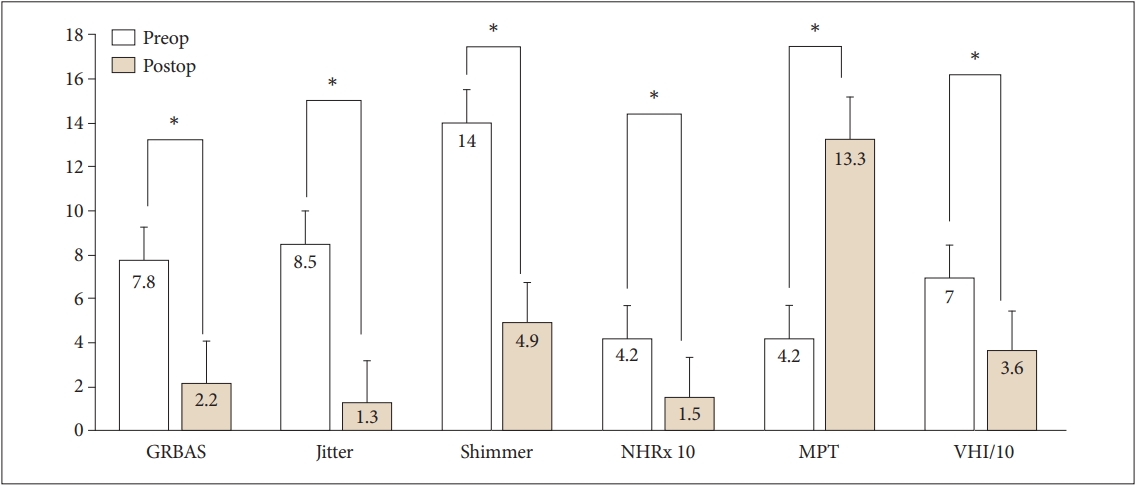
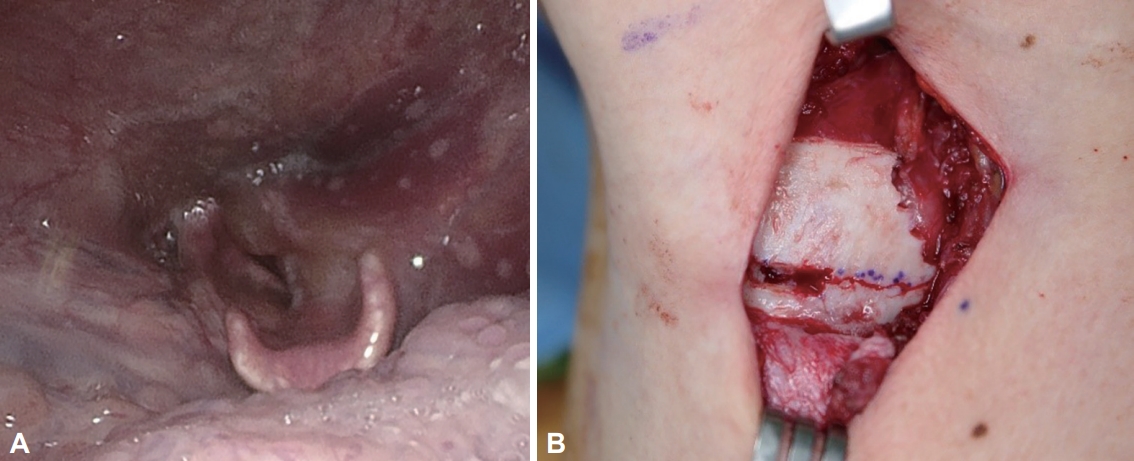
성대마비 환자에서 시행되는 후두골격수술은 수술과정이 성대점막의 외측에서 이루어지기 때문에 성대점막의 손상을 유발하지 않는다. 부분 마취로도 수술이 가능하며 수술 후 음성향상의 효과가 좋고 지속시간이 길다. 제 1형 갑상성형술의 경우 성대 움직임이 회복되었을 때 삽입된 실리콘을 제거할 수 있기 때문에 가역적인 수술이라 할 수 있다. 또한 다른 종류의 후두골격수술을 복합적으로 시행할 수 있어 음성향상을 극대화 시킬 수 있다[19]. 저자는 피열연골내전술을 시행하는 경우 가능하면 제 1형 갑상성형술을 동시에 시행하는데, 12명의 환자에서 동시 수술을 시행 후 1년 이상 추적관찰 한 결과 GRBAS 스케일 총점, 주파수변동율, 진폭변동율, 잡음대조화음비, 최대발성시간, 음성장애지수에서 유의하게 향상된 결과를 볼 수 있었다(Fig. 3). 심각한 합병증이 없는 것도 장점이라 할 수 있지만 피열연골내전술을 시행하는 경우 이상와 점막에 부종과 혈종이 발생할 수 있다(Fig. 4). 저자의 경험상 혈종으로 인해 호흡곤란이 발생한 경우도 있기 때문에 특히 혈액응고장애가 있는 환자에서는 주의를 요한다[20].
후두골격수술의 비교연구
일측성 성대마비의 치료를 위한 후두골격수술 각각의 효과를 비교한 연구는 많지 않다. 제 1형 갑상성형술만 시행한 경우와 피열연골내전술을 동시에 시행한 경우를 비교하였을 때, 앞쪽 성문틈을 교정하는 데는 두 군에 차이가 없었지만 뒤쪽 성문틈은 피열연골내전술을 동시에 시행하는 경우만 교정이 가능하였다. 하지만 두 군의 수술 후 청지각적 음성평가 결과에서는 유의한 차이가 없었다[9]. 체계적 문헌고찰을 통해 제 1형 갑상성형술, 주사후두성형술, 피열연골내전술, 신경재지배술을 비교하였을 때 청지각적검사, 음향검사, 삶의 질 평가, 내시경소견 등에서 치료 방법에 따른 유의한 차이는 없었다[21]. 하지만 이러한 결과의 해석에 있어서 분석에 사용된 대개의 연구가 후향적이며, 각 연구의 모집단이 크지 않고 균일하지 않다는 점을 고려해야 한다. 성대마비 치료를 위한 후두골격수술 각각의 구체적 적응증은 아직 마련되지 않은 상태이며, 추후 이러한 주제에 대한 다기관 연구가 필요할 것으로 사료된다.
결 론
후두골격수술은 일측성 성대마비 환자의 음성향상을 위해 시행되는 신뢰할 만한 수술법으로 많은 연구를 통해 효과가 입증되어 왔다. 후두골격수술은 부분마취 하에서 시행할 수 있으며 음성향상 효과를 높이기 위해 복합적인 수술이 가능하다. 그 중 제 1형 갑상성형수술은 가역적인 수술이며, 피열연골내전술은 후성문 틈이 크거나 성대간 위상차가 있을 때 더욱 유용하다. 후두골격수술에서 심각한 합병증은 드물지만 부종이나 혈종에 의한 호흡곤란이 발생할 수 있음을 유념해야 한다. 술기의 어려움이 있을 수 있지만 최근 다양한 변형적 시도가 보고되고 있으며, 추후 더 나은 치료법들이 소개되기를 기대한다.