ņä£ļĪĀ
ņĢĀņä▒(hoarseness)ņØä ņŻ╝ ĒśĖņåīļĪ£ ļé┤ņøÉĒĢśļŖö ĒÖśņ×ÉņØś ņĀłļ░ś ņØ┤ņāüņØ┤ ņä▒ļīĆņØś ņ¢æņä▒ ļ│æļ│Ćņ£╝ļĪ£ ņ¦äļŗ©ļÉśņ¦Ćļ¦ī ļ░śļō£ņŗ£ ņĢģņä▒ ņóģņ¢æ, ņäĀņ▓£ņä▒ ĻĖ░ĒśĢ, ņŚ╝ņ”Ø, ņŗĀĻ▓ĮņØś ņØ┤ņāü ļō▒ļÅä Ļ░Éļ│äļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż[1]. ņä▒ļīĆ ĒÅ┤ļ”Į, ņä▒ļīĆ Ļ▓░ņĀł, ļØ╝ņØĖņ╝Ć ļČĆņóģ, ņä▒ļīĆ ļéŁņóģ ļō▒ņØś ņ¢æņä▒ ņĀÉļ¦ē ņ¦łĒÖśņØĆ ļ│æļ│ĆņØ┤ ņ×æĻ│Ā Ēæ£ļ®┤ņØ┤ ļ¦żļüłĒĢśļ®░ Ļ▓ĮĻ│äĻ░Ć ļ¬ģĒÖĢĒĢ£ ĒŖ╣ņ¦ĢņØ┤ ņ׳ņ£╝ļ®░ ĒøäļæÉĻ▓Į Ļ▓Ćņé¼ņÖĆ ĒøäļæÉ ņŖżĒŖĖļĪ£ļ│┤ņŖżņĮöĒö╝ļź╝ ĒåĄĒĢ┤ ņĢģņä▒ ņóģņ¢æĻ│╝ Ļ░Éļ│äĒĢ┤ņĢ╝ ĒĢ£ļŗż[2]. ņØ╝ļ░śņĀüņ£╝ļĪ£ ĒśłĻ┤ĆĻĄ¼ņĪ░(vasculature), ņÖĖļ▓łĒśĢ(exophytic) ļ│æļ│Ć, ĻČżņ¢æņä▒(ulcerative) ļ│æļ│ĆņØĆ ņĢģņä▒ Ļ░ĆļŖźņä▒ņØä ņŗ£ņé¼ĒĢśņ¦Ćļ¦ī ņĀĢĒÖĢĒĢ£ ņ¦äļŗ©ņØä ņ£äĒĢ┤ņä£ļŖö ņĪ░ņ¦üļ│æļ”¼Ļ▓Ćņé¼Ļ░Ć ļÅÖļ░śļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż[2,3].
ņä▒ļīĆ ļéŁņóģņØĆ ņä▒ļīĆ ĒÅ┤ļ”Į, Ļ▓░ņĀł, ļØ╝ņØĖņ╝Ć ļČĆņóģ ļō▒ ļŗżļźĖ ņ¢æņä▒ ņĀÉļ¦ē ņ¦łĒÖśņŚÉ ļ╣äĒĢ┤ ĻĘĖ ļ╣łļÅäļŖö ņĀüņ¦Ćļ¦ī ņāüļīĆņĀüņ£╝ļĪ£ ņØ┤ņżæņØī(diplophonia), ļ░£ņä▒ņĀ£ĒĢ£(voice limitation) ļō▒ ņŗ¼ĒĢ£ ņØīņä▒ ļ│ĆĒÖöļź╝ ņØ╝ņ£╝Ēé©ļŗż. ļśÉĒĢ£ ļŗżļźĖ ņ¢æņä▒ ņĀÉļ¦ē ņ¦łĒÖśĻ│╝ Ļ░Éļ│äņØ┤ Ēלļōżņ¢┤ ņĪ░ņ¦üļ│æļ”¼Ļ▓Ćņé¼ļź╝ ĒåĄĒĢ┤ ņ¦äļŗ©ļÉśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż[4]. ņĪ░ņ¦üļ│æļ”¼ĒĢÖņĀüņ£╝ļĪ£ ņä▒ļīĆ ļéŁņóģņØĆ ņżæņĖĄņØś ĒÄĖĒÅēņāüĒö╝ļĪ£ ļæśļ¤¼ņŗĖņØĖ ņ£ĀĒæ£Ēö╝ņóģ(epidermoid cyst)Ļ│╝ ņĀÉņĢĪņä▒ ņāüĒö╝ļĪ£ ļæśļ¤¼ņŗĖņØĖ ņĀĆļźśļéŁ(mucous retention cyst)ņ£╝ļĪ£ ļČäļźśĒĢśļ®░, ņĀĆļźśļéŁņØ┤ ņ£ĀĒæ£Ēö╝ņóģļ│┤ļŗż ļŹö ĒØöĒĢśĻ▓ī ļ░£ņāØĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. ņ£ĀĒæ£Ēö╝ņóģņØĆ ņØ┤ĒĢÖņĀü Ļ▓Ćņé¼ņāü ĒØ░ņāēņØä ļØĀĻ│Ā ļ│┤ļŗż ļ░śņ¦ØĻ▒░ļ”¼ļŖö ņ¢æņāüņØä ļ│┤ņŚ¼ ņłĀ ņĀäņŚÉ ņä▒ļīĆ ĒÅ┤ļ”ĮņØ┤ļéś Ļ▓░ņĀł ļō▒ņ£╝ļĪ£ ņśżņØĖļÉśļŖö Ļ▓ĮņÜ░Ļ░Ć ņĀüņ£╝ļéś, ņĀĆļźśļéŁņØś Ļ▓ĮņÜ░ ņ£ĀĒæ£Ēö╝ņóģņŚÉ ļ╣äĒĢ┤ ņāēĻ╣öņØ┤ļéś ņ¢æņāüņØ┤ ļÜ£ļĀĘĒĢśņ¦Ć ņĢŖņĢä ņä▒ļīĆ ĒÅ┤ļ”Į, Ēś╣ņØĆ ņä▒ļīĆ ļČĆņóģņ£╝ļĪ£ ņśżņØĖļÉśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż[5]. ĒśĢĒā£ĒĢÖņĀü ĻĄ¼ļČäņŚÉ ņ׳ņ¢┤ ĒĢ£Ļ│äĻ░Ć ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ ņä▒ļīĆ ļéŁņóģņ£╝ļĪ£ ņØśņŗ¼ļÉśņŚłļŹś ļ│æļ│ĆņØ┤ ņĪ░ņ¦üļ│æļ”¼Ļ▓Ćņé¼ņāü ļŗżļźĖ ņ¢æņä▒ ņĀÉļ¦ē ņ¦łĒÖśņ£╝ļĪ£ ņ¦äļŗ©ļÉśļŖö Ļ▓ĮņÜ░ļŖö ļ╣äĻĄÉņĀü ĒØöĒĢśļéś ņä▒ļīĆ ļéŁņóģņØä ĒżĒĢ©ĒĢ£ ņ¢æņä▒ ņĀÉļ¦ē ņ¦łĒÖśņØ┤ ņĢģņä▒ ņóģņ¢æĻ│╝ ĒĢ©Ļ╗ś ņ¦äļŗ©ļÉśļŖö Ļ▓ĮņÜ░ļŖö ĻĘ╣Ē׳ ļō£ļ¼╝ļŗż. ļ│Ė ņĀĆņ×ÉļōżņØĆ ĒøäļæÉĻ▓Į Ļ▓Ćņé¼, ĒøäļæÉ ņŖżĒŖĖļĪ£ļ│┤ņŖżņĮöĒö╝ņāü ņä▒ļīĆ ļéŁņóģ ņåīĻ▓¼ņØä ļ│┤ņŚ¼ ĒøäļæÉļ»ĖņäĖņłśņłĀņØä ņŗ£Ē¢ēĒĢśņśĆņ£╝ļéś ņĄ£ņóģ ņĪ░ņ¦üļ│æļ”¼Ļ▓Ćņé¼ņāü ņä▒ļīĆ ļéŁņóģ ļé┤ļČĆņŚÉņä£ ĒÄĖĒÅēņäĖĒżņĢöņóģņØ┤ ĒĢ©Ļ╗ś ļ░£ņāØĒĢ£ ņ”ØļĪĆļź╝ ņ▓┤ĒŚśĒĢśņśĆĻĖ░ņŚÉ ļ¼ĖĒŚī Ļ│Āņ░░Ļ│╝ ĒĢ©Ļ╗ś ļ│┤Ļ│ĀĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ņ”ØļĪĆ
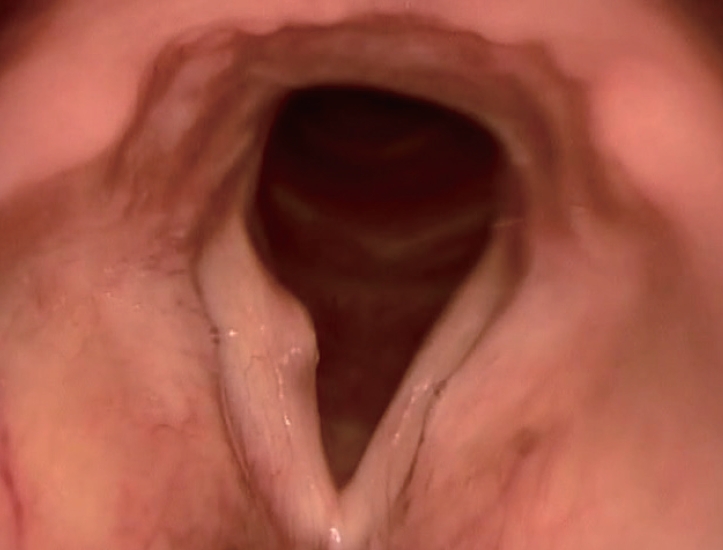
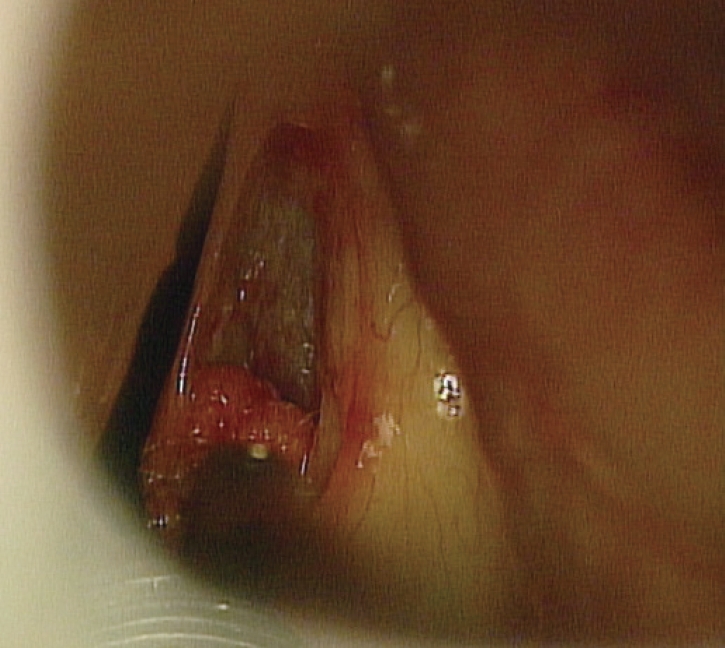
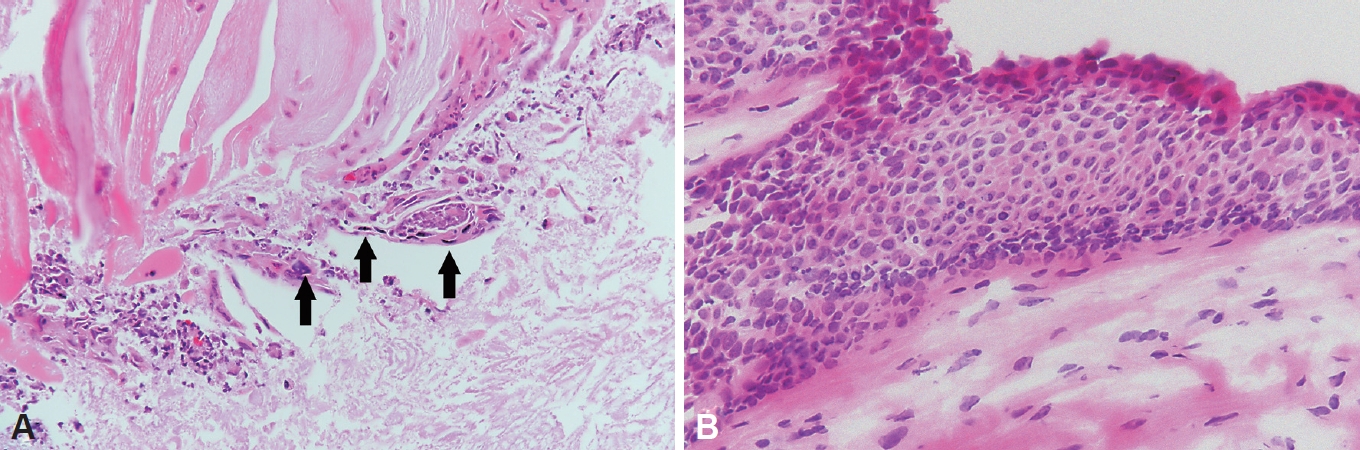
53ņäĖ ļé©ņ×É ĒÖśņ×ÉĻ░Ć 1ļŗ¼ ņĀäļČĆĒä░ ņŗ£ņ×æļÉ£ ņĢĀņä▒ņØä ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢśņśĆļŗż. ĒÖśņ×ÉļŖö 30Ļ░æļģäņØś ĒØĪņŚ░ļĀźņØ┤ ņ׳ņŚłņ£╝ļ®░ ņØīņŻ╝ļĀźņØĆ ņŚåņŚłĻ│Ā ņ¦üņŚģņāü ņØīņä▒ ļé©ņÜ®ļĀźņØ┤ ņ׳ņŚłļŗż. ĒøäļæÉĻ▓Į Ļ▓Ćņé¼ņāü ņÜ░ņĖĪ ņ¦äņä▒ļīĆ ņżæļ░ś 1/2 ņ¦ĆņĀÉņŚÉņä£ ņĢĮ 2~3 mmņØś ļŗ©ņØ╝ ļéŁņóģ ĒśĢĒā£ņØś ņóģļ¼╝ņØ┤ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░(Fig. 1), ņŻ╝ņ£äņØś ĒøäļæÉĻ░£(epiglottis), ņ¢æņĖĪ ņØ┤ņāüņÖĆ(pyriform sinus), Ēö╝ņŚ┤ņŚ░Ļ│©(arytenoid cartilage) ļō▒ņŚÉņä£ļŖö ņØ┤ņāü ņåīĻ▓¼ņØ┤ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż. ĒøäļæÉ ņŖżĒŖĖļĪ£ļ│┤ņŖżņĮöĒö╝ņāü ņóģļ¼╝ ļČĆļČäņŚÉņä£ ņĀÉļ¦ēņØś ĒīīļÅÖņØ┤ ļŗ©ņĀłļÉśļŖö ņä▒ļīĆ ļéŁņóģņŚÉ ļČĆĒĢ®ļÉśļŖö ņåīĻ▓¼ņØ┤ ļéśĒāĆļé¼ļŗż. ņØīņä▒ Ļ▓Ćņé¼ņāü ĻĖ░ļ│ĖņŻ╝Ēīīņłś 118.606 Hz, ņŻ╝Ēīīņłś ļ│ĆļÅÖļźĀ 7.77%, ņ¦äĒÅŁ ļ│ĆļÅÖļźĀ 13.65%, ņ×ĪņØī ļīĆ ņĪ░ĒÖöņØīļ╣ä 0.927ņØ┤ņŚłļŗż. ņĀäņŗĀļ¦łņĘ©ĒĢśņŚÉ ĒøäļæÉļ»ĖņäĖņłśņłĀņØä ņŗ£Ē¢ēĒĢśņśĆĻ│Ā ļ│æļ│Ć ņÖĖņĖĪņŚÉ ņä▒ļīĆņØś ņ×Éņ£ĀņŚ░Ļ│╝ ĒÅēĒ¢ēĒĢśĻ▓ī ņĀłĻ░£ļź╝ ļäŻņ¢┤ ļ»ĖņäĖĒö╝ĒīÉņØä ļōżņ¢┤ ņś¼ļ”░ Ēøä ņä▒ļīĆ ņĀÉļ¦ēņØĆ ļ│┤ņĪ┤ĒĢśļ®░ ņä▒ļīĆ ļé┤ ļéŁņóģņØä ļģĖņČ£ĒĢśņśĆļŗż. Ēö╝ĒīÉņØä ļōżņ¢┤ņś¼ļ”¼ļ®┤ņä£ ļ╣äĻĄÉņĀü Ļ▓ĮĻ│äĻ░Ć ļ¬ģĒÖĢĒĢ£ ļéŁņóģ ĒśĢĒā£ņØś ņóģļ¼╝ņØä ņĀ£Ļ▒░ĒĢśņśĆņ£╝ļ®░ ņä▒ļīĆ ņĀÉļ¦ē Ēö╝ĒīÉņØä ļ│┤ņĪ┤ĒĢśņŚ¼ ņłśņłĀņØä ņóģļŻīĒĢśņśĆļŗż(Fig. 2). ņłĀ Ēøä ņĪ░ņ¦üļ│æļ”¼Ļ▓Ćņé¼ņāü ņä▒ļīĆ ļéŁņóģ ļé┤ļČĆņŚÉ ņ╝ĆļØ╝Ēŗ┤ņØä ĒśĢņä▒ĒĢśļŖö ļ╣äņĀĢĒśĢ ĒÄĖĒÅēņāüĒö╝ņäĖĒżļōżņØ┤ Ļ┤Ćņ░░ļÉśņ¢┤ Ļ│ĀļČäĒÖöĒśĢ ĒÄĖĒÅēņäĖĒżņĢöņóģ(well-differentiated squamous cell carcinoma)ņ£╝ļĪ£ ņ¦äļŗ©ļÉśņŚłļŗż(Fig. 3A). ņØ┤Ēøä ļ│æĻĖ░ ņ¦äļŗ©ņØä ņ£äĒĢ┤ ņ¢æņĀäņ×Éļ░®ņČ£ļŗ©ņĖĄņ┤¼ņśüĻ│╝ Ļ▓ĮļČĆ ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśüņØä ņŗżņŗ£ĒĢśņśĆņ£╝ļ®░ Ļ▓ĮļČĆ ņ×äĒīīņäĀ ļ░Å ļŗżļźĖ ņןĻĖ░ļĪ£ņØś ņĀäņØ┤ ņåīĻ▓¼ņØĆ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢä ļ│æĻĖ░ļŖö 1ĻĖ░(T1aN0M0)ņśĆļŗż. ņ×öņŚ¼ ĒÄĖĒÅēņäĖĒżņĢöņóģņØś ĻĘ╝ņ╣śļź╝ ņ£äĒĢ┤ 2ņŻ╝ ļÆż ņØ┤ņé░ĒÖöĒāäņåī ļĀłņØ┤ņĀĆļź╝ ņØ┤ņÜ®ĒĢ£ ņä▒ļīĆņĀłņĀ£ņłĀ(laser cordectomy type III)ņØä ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░ ņłĀ Ēøä ņĪ░ņ¦üļ│æļ”¼Ļ▓Ćņé¼ņāü ņĀłņĀ£ ļ│ĆņŚ░ņØś ņ╣©ļ▓öņØĆ ņŚåņŚłņ£╝ļ®░ ņĀłņĀ£ ņĪ░ņ¦üņŚÉņä£ļŖö ņāüĒö╝ ļé┤ ĒÄĖĒÅēņāüĒö╝ņĢöņóģ(squamous cell carcinoma in situ)ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 3B). ņłĀ Ēøä 6Ļ░£ņøöĻ░ä ņÖĖļל ĒåĄĒĢ┤ ņ×¼ļ░£ ņåīĻ▓¼ ņŚåņØ┤ Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ ņżæņØ┤ļŗż.
Ļ│Āņ░░
ņĢĀņä▒ņØś ņøÉņØĖņØĆ Ļ░ÉĻĖ░ļČĆĒä░ ņĢģņä▒ ņóģņ¢æĻ╣īņ¦Ć ļ¦żņÜ░ ļŗżņ¢æĒĢśļŗż[6]. ņ×äņāüņŚÉņä£ ņŗ£Ē¢ēļÉśļŖö ĒøäļæÉĻ▓Į Ļ▓Ćņé¼ļŖö ņ¦äļŗ©ņŚÉ Ēü░ ļÅäņøĆņØä ņŻ╝ļ®░ ņØ╝ļ░śņĀüņ£╝ļĪ£ ņóģļ¼╝ņØś Ēü¼ĻĖ░Ļ░Ć ņ×æĻ│Ā Ēæ£ļ®┤ņØ┤ ļ¦żļüłĒĢśĻ│Ā Ļ▓ĮĻ│äĻ░Ć ļ¬ģĒÖĢĒĢśļ®┤ ņ¢æņä▒ ņĀÉļ¦ē ņ¦łĒÖśņØä ņØśņŗ¼ĒĢ┤ņĢ╝ ĒĢśļ®░ ĒśłĻ┤ĆĻĄ¼ņĪ░, ņÖĖļ▓łĒśĢ ļ│æļ│Ć, ĻČżņ¢æņä▒ ļ│æļ│ĆņØ┤ ļ│┤ņØ┤ļ®┤ ņĢģņä▒ ņóģņ¢æņØä ņØśņŗ¼ĒĢ┤ņĢ╝ ĒĢ£ļŗż[2,3]. ļśÉĒĢ£ ļ░▒ļ░śņ”Ø(leukoplakia), Ļ░üĒÖöņ”Ø(keratosis), ņ£ĀļæÉņóģņ”Ø(papillomatosis)ņØĆ ļīĆĒæ£ņĀüņØĖ ņĀäņĢöņä▒ ļ│æņåīņØ┤ļ®░ Ļ░üĻ░ü ĒśĢĒā£ĒĢÖņĀü ĒŖ╣ņ¦ĢņØ┤ ņ׳ņ¢┤ ļŗżļźĖ ļ│æļ│ĆĻ│╝ ņ£ĪņĢłņĀüņ£╝ļĪ£ ĻĄ¼ļČäĒĢĀ ņłś ņ׳ļŗż[6]. ņä▒ļīĆ ņóģļ¼╝ņØś ĒÖĢņ¦äņØĆ ņĪ░ņ¦üļ│æļ”¼ĒĢÖņĀü Ļ▓Ćņé¼ļź╝ ĒåĄĒĢ┤ ņØ┤ļŻ©ņ¢┤ņ¦Ćņ¦Ćļ¦ī ņä▒ļīĆņØś ņ¢æņä▒ ņĀÉļ¦ē ņ¦łĒÖśĻ│╝ ņĢģņä▒ ņóģņ¢æņØĆ ņØ╝ņ░©ņĀüņ£╝ļĪ£ ĒøäļæÉĻ▓Į Ļ▓Ćņé¼, ĒøäļæÉ ņŖżĒŖĖļĪ£ļ│┤ņŖżņĮöĒö╝ļź╝ ĒåĄĒĢ┤ ĻĄ¼ļČäĒĢĀ ņłś ņ׳ļŗż.
ņŗżņĀ£ļĪ£ ĒøäļæÉĻ▓Į Ļ▓Ćņé¼, ĒøäļæÉ ņŖżĒŖĖļĪ£ļ│┤ņŖżņĮöĒö╝ņāü ņä▒ļīĆ ņ¢æņä▒ ņĀÉļ¦ē ņ¦łĒÖśņØ┤ ņØśņŗ¼ļÉśņŚłļŖöļŹ░ ņĪ░ņ¦üļ│æļ”¼Ļ▓Ćņé¼ļź╝ ĒåĄĒĢ┤ ņĢģņä▒ ņóģņ¢æņ£╝ļĪ£ ņ¦äļŗ©ļÉ£ ņśłļŖö ļō£ļ¼╝ļŗż. ĒŖ╣Ē׳ ņä▒ļīĆ ļéŁņóģņŚÉņä£ ĒÄĖĒÅēņäĖĒżņĢöņóģņØ┤ ļ░£ņāØĒĢ£ ņ”ØļĪĆļŖö ĻĄŁļé┤ņÖĖņŚÉ ņĢäņ¦ü ļ│┤Ļ│ĀļÉ£ ļ░ö ņŚåļŗż. ņĢģņä▒ ņóģņ¢æ ņżæ ĒøäļæÉ ņ£Īņóģņ¢æ ņāüĒö╝ņĢö(sarcomatoid carcinoma)ņØĆ ļīĆļČĆļČä ĒÅ┤ļ”Įņ¢æ(polypoid) ļśÉļŖö ņ£ĀĻ▓ĮĒśĢ(pendunculated) ņ¢æņāüņØä ļ│┤ņØ┤ļ®░ ņä▒ļīĆ ņ╣©ļ▓ö ņŗ£ ņä▒ļīĆ ĒÅ┤ļ”Įņ▓śļ¤╝ ļ│┤ņØ╝ ņłś ņ׳ņ¢┤ ņä▒ļīĆ ĒÅ┤ļ”Įņ£╝ļĪ£ ņśżņØĖļÉ£ ņ”ØļĪĆĻ░Ć ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ļŗż[7].
ļ│Ė ņ”ØļĪĆņŚÉņä£ ĒÖśņ×ÉļŖö 30Ļ░æļģäņØś ĒØĪņŚ░ļĀźĻ│╝ ņØīņä▒ņØś Ļ│╝ļÅäĒĢ£ ņé¼ņÜ® Ļ│╝Ļ▒░ļĀźņØ┤ ņ׳ņŚłņ£╝ļ®░ ņ¦äņä▒ļīĆņŚÉņä£ ļŗ©ņØ╝ ļéŁņóģ ĒśĢĒā£ņØś ņóģļ¼╝ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż. ĒśĢĒā£ĒĢÖņĀüņ£╝ļĪ£ ņä▒ļīĆņŚÉņä£ņØś ļÅīņČ£ņØ┤ ļ»Ėļ»ĖĒĢśĻ│Ā ĒøäļæÉ ņŖżĒŖĖļĪ£ļ│┤ņŖżņĮöĒö╝ņāü ļéŁņØś ĒśĢĒā£ļź╝ ļÜ£ļĀĘĒĢśĻ▓ī ļ│┤ņØ┤ļ®░ ĒÖśņ×ÉĻ░Ć ņØīņä▒ ļé©ņÜ®ļĀźņØ┤ ņ׳ņ¢┤ ņä▒ļīĆ ļéŁņóģņ£╝ļĪ£ ĒīÉļŗ©ĒĢśĻ│Ā ĒøäļæÉļ»ĖņäĖņłśņłĀņØä ņŗ£Ē¢ēĒĢśņśĆļŗż. ĒĢśņ¦Ćļ¦ī ņĪ░ņ¦üļ│æļ”¼Ļ▓Ćņé¼ņāü ņä▒ļīĆ ļéŁņóģ ļé┤ļČĆņŚÉ Ļ│ĀļČäĒÖöĒśĢ ĒÄĖĒÅēņäĖĒżņĢöņóģņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż. ļ│Ė ņ”ØļĪĆļŖö ņä▒ļīĆ ļéŁņóģņ£╝ļĪ£ ļ│┤ņØ┤ļŖö ņ¢æņä▒ ļ│æļ│Ć ļé┤ļČĆņŚÉņä£ Ļ│ĀļČäĒÖöĒśĢ ĒÄĖĒÅēņäĖĒżņĢöņóģņØĖ ņĢģņä▒ ņóģņ¢æņØ┤ ļÅÖļ░śļÉ£ ņ×äņāüņĀüņ£╝ļĪ£ ņżæņÜöĒĢ£ ļ│┤Ļ│ĀļĪ£ ņé¼ļŻīļÉ£ļŗż. ļ│Ė ņ”ØļĪĆļź╝ ĒåĀļīĆļĪ£ ĒØĪņŚ░ļĀźņØ┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉņä£ļŖö ņä▒ļīĆ ņóģļ¼╝ ļ░£ņāØ ņŗ£ ļŗ©ņØ╝ ņóģļ¼╝ļĪ£ Ēü¼ĻĖ░Ļ░Ć ņ×æĻ│Ā Ēæ£ļ®┤ņØ┤ ļ¦żļüłĒĢśļ®░ Ļ▓ĮĻ│äĻ░Ć ļ¬ģĒÖĢĒĢśļŹöļØ╝ļÅä ĒÄĖĒÅēņäĖĒżņĢöņóģ ļō▒ņØś ĒøäļæÉ ņĢģņä▒ ņóģņ¢æņØś Ļ░ĆļŖźņä▒ņØä ņÖäņĀäĒ׳ ļ░░ņĀ£ĒĢ┤ņäĀ ņĢłļÉśļ®░ ņāØĻ▓Ć ļ░Å ņĪ░ņ¦üļ│æļ”¼ĒĢÖņĀü ĒŖ╣ņ¦ĢņŚÉ ļö░ļźĖ ļ®┤ļ░ĆĒĢ£ ņ¦äļŗ©ņØ┤ ĒĢäņÜöĒĢĀ Ļ▓āņØ┤ļŗż.